Benjamin Pinckney, 46, has dreamed of becoming a physician assistant since just after his 20th birthday.
He had been targeted by a drive-by shooter in Jacksonville, Florida, and hospitalized with two gunshot wounds. During his weeklong hospitalization, he said, a physician assistant changed the course of his life by visiting his hospital bed each day and warning him that Black men with gunshot wounds often end up paralyzed — or worse.
“I used to run the streets, you know, on the wrong sides of the track,” Pinckney said. “He made me promise that I would never come into his ER that way again. That was the last conversation we had, right before I was discharged.”
His goal since then has been to become a physician assistant. Pinckney, who spent most of his career working for New York City’s Department of Sanitation and as an Army Reserve medic, recently took a step toward achieving it. In May, he graduated with departmental honors from Lehman College with a Bachelor of Science degree.
After moving from New York to Prince George’s County, Maryland, he’d planned on applying for physician assistant school this year. But now, he’s worried his dream may be thwarted by new student loan rules.
Starting July 1, the amount of money graduate students will be allowed to borrow from the federal government will be capped. The new student loan limits are part of the GOP’s tax-and-spending legislation known as the One Big Beautiful Bill Act, which President Donald Trump signed into law last year.
The caps are intended to curb the cost of higher education and student loan debt, according to the Trump administration.
But critics widely agree the new limits are too low, especially for students allowed to borrow only $20,500 a year in federal loans due to the law’s controversial definition of a “professional degree.” On June 24, a federal judge temporarily blocked the Department of Education from enforcing that definition. Still, for many students, the new caps won’t cover the combined cost of tuition, housing, and living expenses.
This could leave hundreds of thousands of students who borrow money for graduate school each year at the mercy of private lenders with higher interest rates and fewer repayment options.
Pinckney wants to go to graduate school to become a physician assistant but doesn’t know how he will finance his education as new student loan limits go into effect. (Erica S. Lee for KFF Health News)
Pinckney earned his Bachelor of Science degree from Lehman College this spring. (Erica S. Lee for KFF Health News)
Pinckney estimates he paid at least 90% of his undergraduate tuition out-of-pocket. (Erica S. Lee for KFF Health News)
Some experts and students also worry that the limits will threaten efforts to diversify the healthcare workforce by deterring minorities and people from low-income households from applying to graduate programs. A drop in incoming students could worsen existing rural and primary care shortages, they argue.
Many politicians and loan experts have acknowledged that the cost of higher education needs to be addressed. But the new federal loan limits are “just not going to achieve that goal,” said Todd Pickard, president of the American Academy of Physician Associates, one of several organizations that have sued the Department of Education over the rules.
“It’d be like if you had a hangnail and I cut your whole arm off instead of just taking care of your hangnail,” Pickard said. “The treatment doesn’t match the problem.”
‘A Rock and a Hard Place’
Students working toward what the law describes as “professional degrees” — including trainee doctors, dentists, pharmacists, and chiropractors — will be allowed to borrow up to $200,000 total, and no more than $50,000 a year.
Meanwhile, the median cost of attending a public medical school is nearly $300,000 over four years, while the median cost of a private medical school education exceeds $400,000, according to the Association of American Medical Colleges.
The caps were set even lower for those pursuing other “graduate” degrees, who face a $100,000 borrowing limit for federal loans over the course of their degree programs. The annual limit for this category of students is only $20,500. Students pursuing physical therapy, physician assistant, and nursing degrees were originally included in this group. But according to new guidance issued by the Department of Education on Monday, some of these students will at least temporarily be able to borrow up to the higher limit, according to The Associated Press.
The Department of Education, which has been sued by clinician trade groups and about two dozen states over the new rules, did not respond to questions for this article.
As the law was written, a physician assistant student who completed their degree within the average two to three years would not have been eligible to borrow the full $100,000. Meanwhile, physician assistants typically start their careers with an average debt of $112,000, meaning some could be forced to finance their education with higher-interest private loans.
“I feel like I’m between a rock and a hard place,” said Olivia Trull, 24, who is scheduled to begin the physician assistant program at Northwest University in Kirkland, Washington, this summer. The 28-month program costs $137,000, with about $62,000 in tuition and fees estimated for the first year, she said. That doesn’t include living expenses.
Before the court order, Trull said she qualified for the maximum annual allotment under the new rules of $20,500 in federal loans during her first year of graduate school. The balance would need to be financed through a private lender.
She anticipated she would need up to $100,000 in private loans to finance her graduate degree and would face loan payments of more than $3,000 a month when she was done.
“I have to actually sit down and have a conversation with myself,” Trull said, to consider “if I want to be drowning in debt for the next 10 years of my life.” One private bank offered her a loan with an interest rate of nearly 14%, she said.
Pinckney, who said he finished his undergraduate degree with about $10,000 in federal student loan debt, said some of his friends who have already applied for private student loans have been quoted interest rates as high as 13%. Meanwhile, interest rates for federal loans for graduate students, which are set annually, are currently about 8-9%. Federal loans also offer more flexible repayment options than private loans typically do.
In May, 25 states and the District of Columbia filed a federal lawsuit against the Department of Education over the new rules. The complaint described the law’s “professional degree” definition as “arbitrary and capricious.”
In a separate federal lawsuit filed in June, the American Academy of Physician Associates and the PA Education Association alleged that the new rules deny students the loan amounts needed to attend physician assistant schools. They argue that PA students should be able to access the higher loan limits available to students in medical school and other professional degree programs. (While “physician assistant” and “physician associate” typically refer to the same role, the AAPA adopted the title “physician associate” in 2021 because of “concern that ‘assistant’ does not reflect the important role of PAs in delivering high-quality healthcare to patients.”)
Meanwhile, Trump administration officials have contended the cost of graduate school is too high across the board. Education Secretary Linda McMahon, speaking before a House committee in May about the new limits, said, “It is our overall goal to bring down the cost of college and education.”
Indeed, some experts acknowledge that the new limits may be helpful in bringing down costs. The federal Grad PLUS loan program, established by Congress 20 years ago, did not cap the amount graduate students could borrow in federal loans. That program was eliminated in the One Big Beautiful Bill Act.
“There is considerable evidence that people borrowed more than they really needed to go to school,” said Sandy Baum, a higher education economist and a senior fellow at the Urban Institute.
Already, some graduate programs have lowered tuition prices, Baum said. In May, for example, the University of California-Irvine announced it would lower the cost of its MBA programs by tens of thousands of dollars to fall below the new federal lending thresholds.
And yet Baum doesn’t anticipate many other schools will follow suit.
“I don’t think we’re going to see some dramatic decline in prices,” she said. “I think some programs could close down because they can’t manage.”
‘Tears Have Been Shed’
The new lending limits will also disproportionately affect Black students, Baum said, because they have historically borrowed more than white and Hispanic students.
For some students who borrowed money to finance their undergraduate degrees, the new limits will hit especially hard. Under the new rules, they will be subject to a lifetime limit of $257,000 in federal student loans.
“There will be students who can’t enroll,” Baum said.
Andrei Robu, 26, a medical student at the Medical University of South Carolina, leads the Financial Literacy Interest Group on the Charleston campus. He said many of his peers are worried that the lending limits will make the student body less diverse.
He is also concerned that, because the demand for acceptance into medical school is already so high, schools could prioritize entrance for students from wealthy backgrounds and “still fill up their classes.”
“That’s just not what we want in our physician workforce,” said Robu, who isn’t subject to the new rules as a current student. “We want to represent the population of the country at large.”
Jasmine Vasquez, 26, who has been accepted into the physician assistant program at South College in Atlanta, decided to defer her enrollment until 2027, partly to see if her financing options change. She is worried about taking on too much debt from a private bank.
“Tears have been shed multiple times,” said Vasquez, who is due to give birth in September. “It’s nothing that’s within my control.”
Betsy Mayotte, president of the Institute for Student Loan Advisors, expects the new rules will force some graduates into bankruptcy when they can’t afford to repay private loans.
First, though, she expects enrollment numbers to drop and some graduate programs to close because they can’t recruit enough students. Completion rates will also drop, she expects, as students run into federal loan limits partway through their degree programs.
Beyond that, she predicts healthcare graduates will seek jobs in high-paying specialties, exacerbating shortages in rural and underserved communities.
“They’re going to go where they can make the most money,” Mayotte said.
Pinckney has spent most of his career working for New York City’s Department of Sanitation. But he has dreamed of becoming a physician assistant since he was treated for gunshot wounds at a Jacksonville, Florida, hospital in 1999. (Erica S. Lee for KFF Health News)
Pinckney said he is “not really sure” what the future holds. He paid for most of his undergraduate education by working while he was in school, but that’s typically not possible for full-time physician assistant students.
He has considered applying to a biomedical science graduate program instead, which he estimated would cost about $30,000 — an amount that’s “a lot more doable,” he said. It would allow him to potentially work in a lab or in pharmaceuticals, he said. It’s still aligned with medicine, he said, but it wouldn’t help him realize his goal of working with patients.
“Maybe this thing will blow over,” he said of the new federal loan limits. In the meantime, he’s holding out hope.
“If I can influence one person’s life, that would be my way of paying him forward for what he did,” he said, referring to the physician assistant who inspired him back in 1999. “It’s very hard to pivot from that dream.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Alea Bates wasn’t ready to leave Tallahassee Memorial HealthCare’s main hospital four days after a stranger shot her seven times at close range. Miraculously, hospital records show, none of the bullets damaged her internal organs.
But after surgery, Bates said, she couldn’t get out of bed or walk to the bathroom without help. She complained of intense pain radiating down her left leg, weakness in her knee, and a numbing sensation below it, according to hospital records. Bates, who worked as an Uber Eats driver, didn’t have the strength to drive a car.
Still, Bates said, the hospital told her it was time to go.
“They didn’t do any further X-rays or CTs or MRIs to figure out why my knee was numb,” she said. “And they were just like, you know, ‘It’ll go away.’”
Doctors said she was medically stable, Bates said, and because she had no health insurance, they could not send her to a rehabilitation hospital or a skilled nursing facility, which can charge thousands of dollars a day for such care.
“They were just like, We need the bed for somebody who has insurance,” she said. “That’s of course, you know, what they say without saying it.”
At least one firearm injury is treated in an American emergency room every 30 minutes. Tens of thousands die from their injuries every year. Many more, like Bates, are left to face long recoveries, steep medical debt, and enduring trauma.
How insurance affects the care of gunshot wound victims has remained shrouded in mystery — until now, due to a new analysis by The Trace and KFF Health News of data that Florida hospitals compile to collect payments from insurance companies and file with the state.
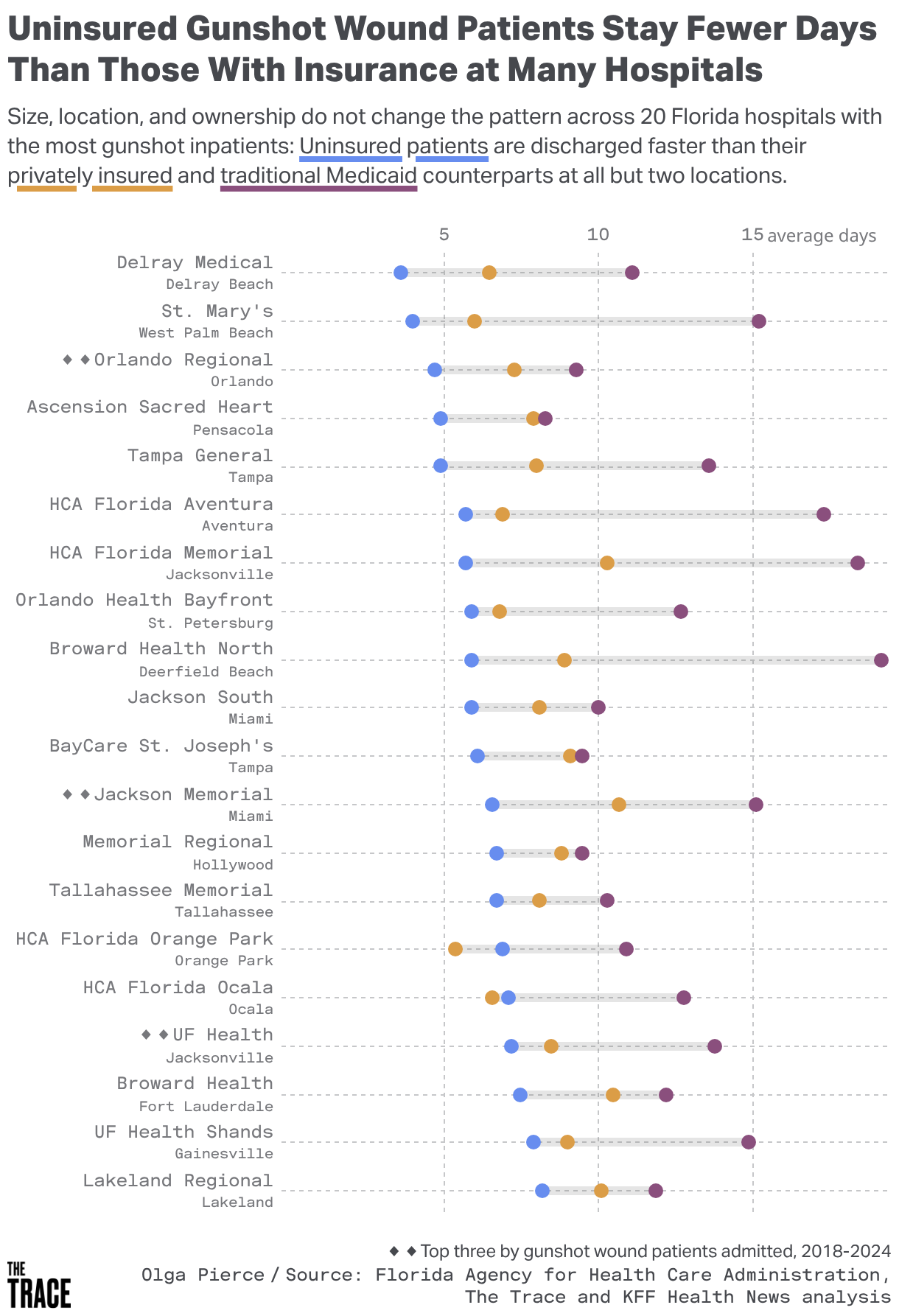
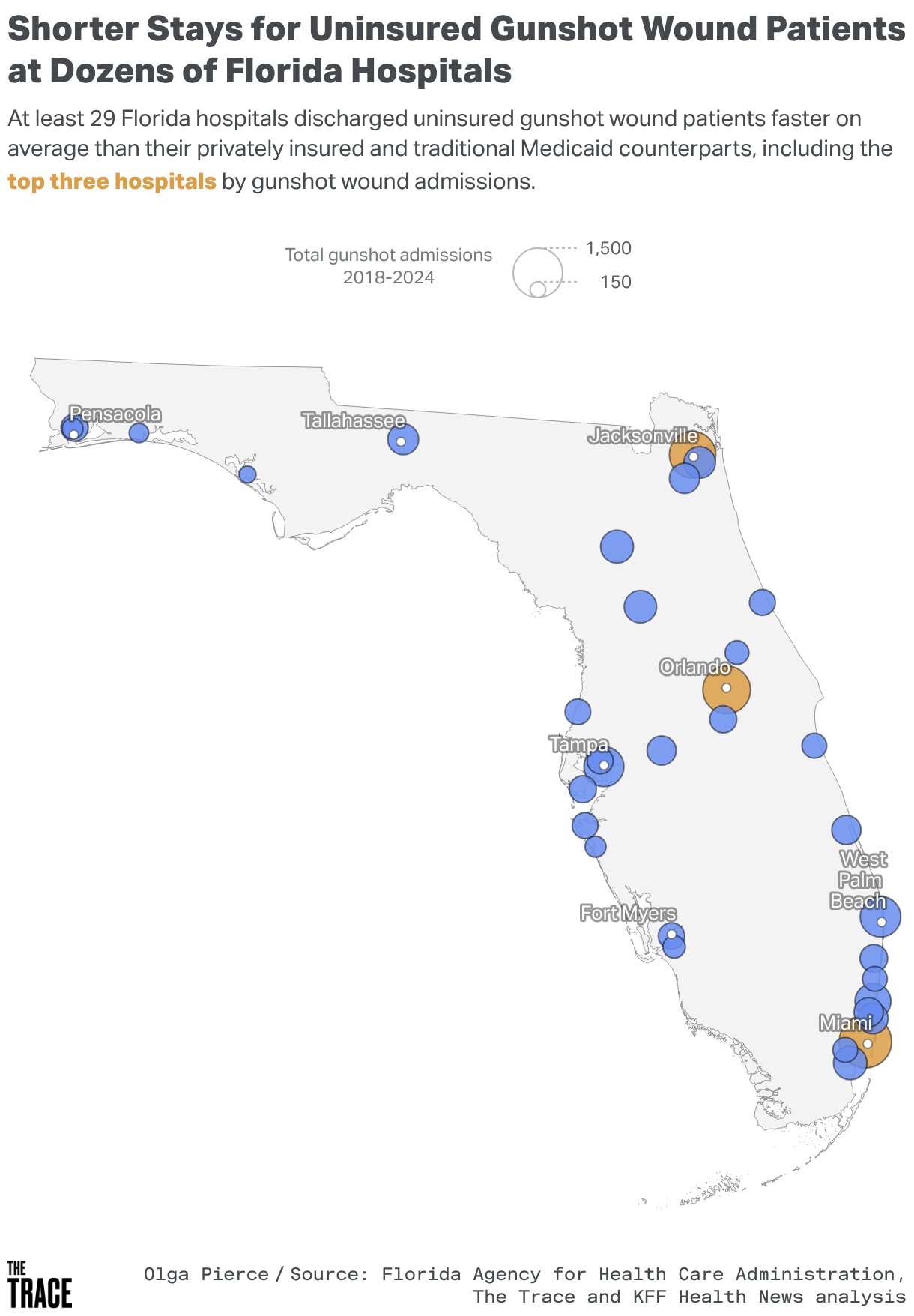
When uninsured patients arrive at hospitals in Florida with gunshot wounds, on average they spend significantly fewer days in the hospital — in some cases half the time — than those with health insurance, according to the data analysis.
Among the most severely injured patients, the uninsured stayed three fewer days in the hospital on average than their counterparts with insurance.
The data was obtained exclusively for this reporting on gun violence hospitalizations in the state, aided by Florida state law.
The newsrooms spent more than a year analyzing the records, which did not identify patients. The data contained patients’ insurance status, their residential ZIP code, their race, and other demographic info. Reporters reviewed academic studies and government documents and interviewed health policy experts, doctors, activists, and victims of gun violence or their relatives.
The results are a first-of-its-kind look at what happens to the insured and the uninsured who are shot and admitted to the hospital for treatment.
Across Florida, the analysis of hospital billing data from 2018 to 2024 obtained from the Florida Agency for Health Care Administration shows:
Uninsured patients make up a quarter of the more than 20,000 gunshot wound hospitalizations identified, making them the largest single group treated for firearm injuries.
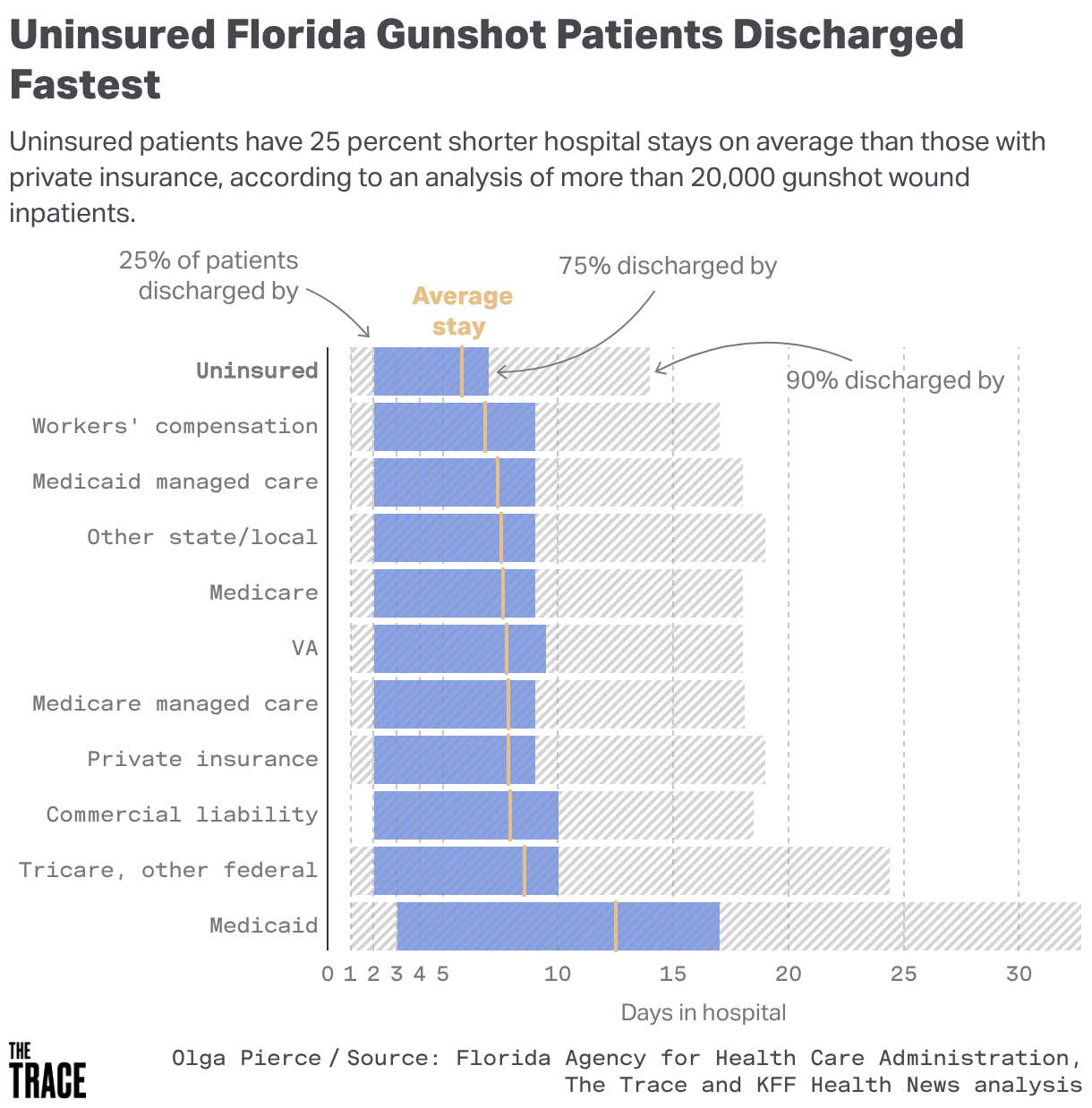
Uninsured gunshot victims had hospital stays of about six days on average, only three-quarters of the time spent by patients with private insurance and less than half the average stay for patients on traditional Medicaid, the public health insurance program for poor and disabled people.
The gap in hospital care persisted regardless of hospital size, location, or ownership type, including at facilities that receive taxpayer money with a mandate to treat all patients regardless of their ability to pay.
Of the gunshot wound patients, nearly half were Black, making the group highly overrepresented. About a quarter of nonwhite patients were uninsured, versus fewer than a fifth of white patients.
The U.S. has more gun violence deaths than other wealthy nations, and no group suffers more than Black Americans like Bates. Black people are far more likely to become victims of a firearm homicide than white people, according to the Johns Hopkins Bloomberg School of Public Health.
Handguns for sale at a gun shop in Delray Beach, Florida. Florida law allows eligible residents to carry a concealed firearm and to openly carry a firearm without a state-issued license. (Joe Raedle/Getty Images)
Patient outreach workers say hospital personnel might perceive gunshot victims as gang members or troublemakers who deserve blame for getting shot. One study found rehab centers refuse to admit gunshot victims more often than other patients, and some medical records from hospitals were littered with racist or insensitive descriptions of patients and their behavior.
The damage can be lasting: Patients who leave the hospital too soon after a traumatic injury have a higher risk of serious complications, including infection, hemorrhage, nerve damage, and death, especially if wounds — and mental health concerns — are left untreated.
Arch Mainous, a University of Florida professor and vice chair for research in community health and family medicine, said there’s evidence that financial incentives drive care — for patients and for hospitals.
Regardless of how often the care team is told to follow quality protocols, Mainous said, “ultimately there’s a business aspect to it, whether the physician is thinking about it or not, whether the nurses think about it or not. But somebody is.”
The Florida data findings come at a time when Republican Gov. Ron DeSantis and state lawmakers have pushed to make guns cheaper and more widely available, despite a 19% increase in gun deaths in the state from 2014 to 2023, and when President Donald Trump’s administration has rolled back legislation from the Joe Biden presidency to curb gun violence and pushed millions of Americansoff health insurance.
Florida Gov. Ron DeSantis at a Hooksett, New Hampshire, gun shop in 2023. DeSantis has pushed to make guns cheaper and more widely available, despite a 19% increase in gun deaths in Florida from 2014 to 2023. (Sophie Park/Bloomberg via Getty Images)
Florida law allows eligible residents to carry a concealed firearm and to openly carry a firearm without a state-issued license. State law also prevents cities and counties from enacting stricter gun control measures.
In early June, Florida Attorney General James Uthmeier asked a federal judge to strike down the state’s three-day waiting period for receiving a purchased gun, arguing it is unconstitutional. Uthmeier’s request is part of a proposed settlement of a lawsuit brought by the National Rifle Association.
KFF Health News and The Trace requested to speak with administrators at nine of Florida’s large hospital systems to ask why the disparities exist. None agreed to an interview.
Sarah Cannon, communications director at Tallahassee Memorial HealthCare, would not agree to an interview or address Bates’ account of her care for gunshot injuries.
“Clinical decisions, including acute medical intervention, readiness for discharge, and post-acute care needs, are guided by the patient’s condition and response to treatment,” she said in an email.
Cannon said the hospital offers support to patients after discharge, including from social workers who coordinate care and access to services including post-acute care placement, home healthcare, and primary care or specialty follow-up.
Bates said she had to coordinate her own care after being released from the hospital. She said nobody called to schedule a follow-up test of her leg’s muscle function, and her medical records show she did not receive one.
“If I had had insurance,” she said, “they would have definitely kept me there for at least another week to work with me on my standing and walking.”
Tallahassee Memorial Hospital, where Bates was admitted after being shot seven times in 2019. She was discharged after four days. (Miguel J. Rodríguez Carrillo/Getty Images)
‘It’s a Business’
Some of Florida’s largest hospitals showed huge differences in length of stay for gun injuries, the KFF Health News-Trace analysis showed. In Miami at Jackson Memorial, the average number of days in the hospital for uninsured patients was 6.6; for those with private insurance, it was 10.7; and for those on traditional Medicaid, it was 15.4. Jackson Memorial did not respond to requests for comment.
Tampa General Hospital reported 4.9 days for uninsured patients, 8 days for those with private insurance, and 13.6 days for Medicaid patients. “To suggest that care decisions for trauma-related patients, and in this case, gun shot victims, are influenced by insurance status is not only absurd, it’s inaccurate,” Amanda Bevis, a hospital spokesperson, said in a written statement. “At Tampa General, every patient is treated equally, based on clinical need and urgency, not insurance coverage.”
And at UF Health Jacksonville, it was 7.2 days for the uninsured, 8.5 days for the privately insured, and 13.8 days for patients on traditional Medicaid. UF Health declined to comment.
Broward Health in Fort Lauderdale reported 7.5 days for uninsured patients, 10.5 days for privately insured patients, and 12.2 days for those on traditional Medicaid. “Insurance status does not impact treatment plans for patients,” Jennifer Smith, a Broward Health spokesperson, said in an email. “Our physicians always proceed in the best interest of the patient regardless of reimbursement or what length of stay may be required.”
Memorial Regional Hospital in Hollywood reported 6.7 days for uninsured patients, 8.8 days for privately insured patients, and 9.5 days for those on traditional Medicaid. Tania Ordaz, a hospital spokesperson, said in an email that she disagreed with the findings: “Treatment decisions are based on the patient’s clinical condition and what is necessary to ensure a safe and appropriate transition of care, not on the patient’s insurance status.”
Trauma surgeons and academics said the Florida data aligns with research nationwide on where gun violence occurs and who’s most affected. Some said they fear the differences contribute to long-standing disparities in America’s healthcare system along the lines of race and class.
The Florida hospital data showed gunshot injuries are concentrated in a handful of ZIP codes marked by poverty, disinvestment, redlining, and other injustices stemming from racial discrimination.
“Why would people without insurance be discharged earlier?” Mainous said. “Because they’re in better health? I think we’ve got a lot of data that would suggest that’s not true.”
Once they leave the hospital, people with commercial insurance or traditional Medicaid are more than twice as likely to receive follow-up care from another provider — such as a rehab center or home health service — as uninsured patients.
Those patients are staying longer, in part, because hospital case managers coordinate their transfers to other facilities, which can be time-consuming and take days.
“You have to go through insurance authorization and approval,” said Rishi Rattan, a trauma surgeon formerly at Jackson Memorial in Miami who now practices in Oregon. He said patients with private insurance might have access to rehab, preventive care, and training for both the patient and their caregiver to “help them transition to a completely new phase of life.”
For patients without insurance, he said, “sometimes our hands are a little bit tied.”
“The hospital is telling us that this patient has to leave the hospital because they’re medically ready,” he said, “and so I guess we’re discharging them to their car or to their tent, and it doesn’t feel right, but I think that would probably explain some of the differences” in length of stay.
Julie Valenzuela, a trauma surgeon at Jackson Memorial, said hospital staff work to ensure that uninsured patients with long recoveries learn to care for wounds and to enlist family help at home.
Valenzuela said the county-owned hospital does not send uninsured patients home to fend for themselves. She goes into neighborhoods and follows up with patients as part of a Miami-Dade County violence intervention program, whose social workers help them access food, employment, and more to heal and feel safe.
“We know that full recovery is beyond just the hospital and even the rehab centers, even the best ones,” Valenzuela said, pointing to housing and navigating the healthcare system as factors.
Wayne Rawlins runs the Miami-Dade program, which connects victims of gun violence with social workers who visit bedside at the hospital and an intensive care unit-trained nurse who visits at home to provide wound care and other services.
Rawlins said young, Black gunshot patients without health insurance are often at a loss when they leave the hospital about how to schedule a follow-up appointment or manage their mental health.
“After they have been shot and they’re getting out of the hospital and they’re still in crisis,” he said, “their concern is more: How am I going to now pay the rent? How am I going to live? Who’s going to take care of me?”
Often, he said, his uninsured clients leave the hospital before they are ready.
“That’s the reality of it: It’s a business,” he said. “It’s like a hotel. You know, checkout time: You got to go. We got to make room for someone, for a next customer.”
How Long Is Long Enough?
Alea Bates said the hospital discharged her with crutches and one prescription: a seven-day supply of the painkiller Percocet.
A family member drove Bates home. She wore a leg brace, with bandages on her back, stomach, hand, forearm, and feet. When she tried to get out of the car, Bates said, her knee gave and she fell.
Surgeons, health policy experts, and researchers say physicians follow evidence-based best practices for treating gunshot wounds and that a shorter hospital stay does not necessarily reflect a lower-level of care.
Elinore Kaufman, an assistant professor of surgery at the University of Pennsylvania who conducts research on violence reduction, offered one explanation.
In a study published in The Journal of Trauma and Acute Care Surgery, Kaufman and colleagues found that patients who were admitted while uninsured but then enrolled in Medicaid during their hospitalization — and who needed ongoing rehabilitative care after discharge — spent more time in the hospital and had higher costs.
“I have personally been in situations where I felt like I did the best I could for a patient, but they would say, ‘You’re kicking me out,’” she said. “Sometimes, what the doctor is telling you doesn’t match what you are feeling in your body.”
But Kaufman said: “I’m not going to tell you hospitals never discriminate. That would not be realistic. I would say it is more indirect.”
Kaufman said she couldn’t judge whether Bates stayed in the hospital long enough because she was not her doctor. Still, she said, Bates “didn’t get what she needed from our healthcare system.”
Unlike many states, Florida excludes most single adults without children, like Bates, from Medicaid eligibility, making it exceedingly uncommon for a Medicaid patient to have been admitted as an uninsured adult.
Gunshot survivors endure bleeding and oozing flesh wounds and pain, and they experience depression and post-traumatic stress disorder. “These experiences are common, but they are not talked about,” Kaufman said. “Mental health is part of the recovery process.”
Recovering the ability to walk or use an arm or a leg after a gunshot wound requires rehab and physical therapy that can be out of financial reach for uninsured patients, said Brian Englum, a pediatric surgeon and an associate professor at the University of Maryland who has found that uninsured patients hospitalized for traumatic injuries have shorter stays than insured patients.
Bates was shot seven times at close range — twice in the back and once each in the pelvis, stomach, left forearm, right thumb, and right foot. (Alea Bates)
Bates took this photo of her left forearm after surgery. (Alea Bates)
A shorter stay, he said, “suggests that these patients are not getting the same level of care, and that’s going to put them at risk for functional deficits down the road.”
He said it is impossible to arrive at a set number of days that any patient should remain in a hospital. Factors include the severity of their injury, their age, and any other illnesses they have.
“We’re looking for that Goldilocks length of stay,” Englum said, “and unfortunately, it is not perfectly defined for any specific admission, and it’s not perfectly defined for any specific patient.”
‘Oh, Shit. He Shot Me.’
Police found Bates lying on the ground in the breezeway of an apartment building the night she was shot seven times after making a food delivery in December 2019. Crime scene photos documented blood and bullet casings from the assault. (Tallahassee Police Department)
Bates had delivered her last order for the night when she was shot. It was December 2019: As she was walking back to her car, she heard two loud bangs. Just kids playing pranks, she thought to herself. Then she turned toward the sound and saw a gun pointed at her.
“In that split second it registered in my mind, like, ‘Oh, shit. He shot me,’” Bates said. “I had some brief, like, burning, but it wasn’t registering in my brain right away what it was.”
Within seconds, Bates said, the stranger emptied the clip of his handgun into her body, even after she fell to the ground. He shot her seven times — twice in the back and once each in the pelvis, stomach, left forearm, right thumb, and right foot.
Bates screamed. She reached for her cellphone to call 911. She said residents came out of their apartments. Someone took her phone to tell the emergency dispatcher the address. Another person pressed towels on her wounds to slow the bleeding. An ambulance rushed her to Tallahassee Memorial.
Bates had descended the stairs of an apartment complex and was walking back to her car when a stranger opened fire. (Tallahassee Police Department)
A bullet hole in the bedroom window of an apartment near the breezeway where Bates was shot in 2019. (Tallahassee Police Department)
Bates said she did not believe race was a factor in the care she received. But she believed that the circumstances surrounding her shooting — that it happened while she was working, and that she did not know the shooter — affected the way doctors and nurses viewed her.
Language in medical records can sometimes signal a bias in clinicians and perpetuate differences in care that patients receive, said Jonathan Jay, an associate professor at the Boston University School of Public Health who conducts research on exposure to gun violence.
Jay said bias based on patients’ race, income, or insurance status can deny some people necessary treatment once they leave the hospital.
He said his research suggests the healthcare system treats gunshot survivors and motor vehicle accident victims differently based on perceptions of “whether the victim was in no way at fault. They made assumptions when a person was violently shot.”
“The results are consistent with what we hear so much from hospital outreach workers for gunshot victims,” he said. “They say there is substantial bias. There is an assumption that they contributed to their condition with risky behavior.”
The preoperative notes in Bates’ medical records describe her as “a pleasant 39-year-old female who sustained multiple gunshot wounds to her abdomen, pelvis and extremities last night after performing Uber Eats delivery.”
Bates said it mattered to her caregivers what she was doing when she was shot.
“The nurses and doctors, they all talk about that stuff,” she said. “They were like, ‘Oh, my God, you were ambushed. That’s so scary.’
“I was working. Like, I don’t know these people. And the fact that they were teenagers, I think that that is what maybe changed the narrative,” she said. “Because I feel a lot of times people blame you for what happened.
“But when I was asked and I told them what happened and my story and how I got there,” she said, “I think just the shock in people’s eyes of like, ‘Oh, my God. So you really were, like, you know, minding your business.’”
She added: “And it also wasn’t in a sketchy part of town, if I can just say that. I was in a predominantly white complex. So I think that’s what saved me.”
Bates was uninsured when surgeons removed bullets and fragments from her body after a stranger shot her seven times. She went home from the hospital after four days with about $60,000 in bills. (Alicia Devine for KFF Health News)
‘Less Than a Human Being’
Bates had received care at the hospital before as an insured patient.
She had lost her job in the legal department of a state agency — along with her insurance — two months before she was shot.
As an uninsured patient, Bates said, “they kind of just dismiss you. It makes you feel like less than a human being.”
She said she felt ignored when she told doctors she didn’t feel safe going home after four days. She said the physical therapist working with her at the hospital had persuaded the facility to let her stay an extra day.
“We would like, as a medical community, I think as a society, to see everybody get the same care,” said Englum, the University of Maryland trauma surgeon. “Regardless of what color their skin is, what insurance status they have — we want them to get appropriate care.”
The reason for racial or ethnic differences in care is hard to tease out, Englum said. Is it that there’s mistrust of the medical system in some Black and Latino communities, leading people to avoid going to rehab because they don’t want to be there? Is it an income issue? Is it that medical providers see some patients and, due to implicit or explicit bias, think, “That’s as good as they’re going to get?”
“Getting that care is what you need to get your full functional outcome back. And if you’re not getting it,” he said, “patients are suffering that didn’t have to.”
At home, Bates said, she depended on family members to help her out of bed, drive her places, even help her feel safe out in public.
“I really didn’t know how to stand or move or walk around,” she said. “I had to figure it out.”
She still fears loud noises, which remind her of being shot. Bates said she and her dog stay indoors on July Fourth and New Year’s Eve.
“The fireworks were going off, and I was paralyzed,” Bates said of her first New Year’s Eve after being shot. “I was literally sitting there crying. My cousin actually came outside and put my noise-canceling headphones on and turned the music on so that I couldn’t hear anymore. That’s the only way that I could move from outside to inside.”
Bates didn’t have the strength to walk after being hospitalized for seven gunshot wounds. Still, after four days, the hospital told Bates it was time to go. (Alicia Devine for KFF Health News)
Bates said her follow-up care included getting her stitches removed at an orthopedic clinic that has physicians who work at the hospital and had performed the initial surgery.
During the visit, Bates said, the orthopedic clinic’s staff reminded her of the unpaid balance from her surgery, which was about $1,200 for physician services. She still owed the hospital $52,000 for treatment, according to her medical bills, and an additional $5,300 for the anesthesiologist. Bates was not working at the time.
Bates said a community outpatient clinic provided physical therapy at a reduced cost and that the victim advocate unit at the Tallahassee Police Department helped find her mental health counseling and get her financial aid from Florida’s compensation fund for crime victims.
By 2021, Bates developed a cyst on the gunshot wound to her right thumb, which required surgery. But, she said, the clinic would not perform the surgery until she paid her $1,200 balance. She said friends paid the bill so she could have the surgery.
Bates’ knee bothered her. “Even with going through physical therapy,” she said, “it was still like I couldn’t feel it.”
Bates said she now has private health insurance that pays for her mental health therapy. She pays for physical therapy out-of-pocket.
“It’s crazy that in this country somebody else can hurt you,” Bates said, and “you have to pay for what they did to you.”
“So it’s like you’re triple-paying: You’re paying every day mentally, you’re paying with the bills, and you’re paying by them saying, We know that this is not your fault, but we still have to make our money.”
KFF Health News data editor Holly K. Hacker contributed to this report.
This article was produced in partnership with The Trace, a nonprofit newsroom covering gun violence in America. Sign up for its newsletters here.
Methodology
The Trace and KFF Health News examined more than 20 million inpatient hospitalizations in Florida from 2018 to 2024, using data obtained from the Florida Agency for Health Care Administration. We identified 20,255 gunshot wound-related visits using the Centers for Disease Control and Prevention’s injury surveillance case definition, which relies on ICD-10-CM diagnosis codes. We limited the analysis to initial encounters and excluded patients who died in the hospital or left against medical advice. We excluded cases in the top 1% for hospital length of stay (68 days or more) to prevent these outliers from disproportionately influencing results.
Our primary finding compares the average length of stay of uninsured patients with that of privately insured patients. We chose privately insured patients as the reference group because many researchers believe their care on average is long enough to be effective but not longer than medically necessary. Overall, uninsured patients had hospital stays that were about 25% shorter on average than privately insured patients’ and 50% shorter than those of patients on traditional Medicaid. In most cases we also found that, within the same hospital, uninsured patients had shorter stays than privately insured ones.
To assess whether age or injury severity explained the shorter lengths of stay for uninsured patients, we calculated injury severity scores and fit regression models for Florida’s highest-volume gunshot wound hospitals. We found that, in nearly all cases, the gap narrowed slightly but did not disappear.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
A major Medicare Advantage company has paid the government more than $342 million to help settle allegations that it overcharged the federal healthcare program for years.
Elevance Health, which covers about 2 million people on Medicare, sent the money to the Centers for Medicare & Medicaid Services via wire transfer on May 27, court records show. Government lawyers disclosed the payment in a June 22 court filing.
In an email to CMS staff, Elevance described the money as a “remittance of the total overpayment amount” estimated by government audits, court records show. Company spokesperson Leslie Porras told KFF Health News in a statement that Elevance Health “continues to engage in constructive dialogue” with CMS. “We remain optimistic that a resolution can be reached and value our longstanding relationship with CMS,” she said.
The payment was made in response to a CMS enforcement action in February, in which the agency threatened to halt enrollments in Elevance Medicare Advantage plans unless the company corrected what CMS called “substantial and persistent noncompliance” with federal regulations that require health plans to submit accurate billing data and return any overpayments when they are discovered.
It appears to be the first time CMS has successfully pressured a Medicare Advantage health plan to pay back tens of millions of dollars in alleged overpayments — even though agency officials have known for years that many health plans have overbilled the program, according to audits by government staff.
“I’ve never heard of something like this before,” said David Lipschutz, an attorney with the Center for Medicare Advocacy, a nonprofit public interest law firm. “Usually plans seem to tie everything up and try to delay any repayment of anything for years.”
David Meyers, an associate professor at the Brown University School of Public Health, called the payment “substantial” and “a step in the right direction” toward holding the industry accountable.
“It’s a big win for CMS to get that much,” he said.
More than 35 million Americans, about 55% of people on Medicare, have signed up for the private Advantage health insurance plans, which offer extra benefits, such as hearing aids and dental coverage, that traditional Medicare doesn’t cover.
Joining the plans may also prove cheaper for patients than purchasing a supplemental insurance policy that covers gaps in traditional Medicare.
Whether Medicare Advantage is a good deal for taxpayers is hotly debated, however.
The health plans have been the target of dozens of whistleblower lawsuits and government investigations alleging they often exaggerate how sick patients are to improperly boost their payments, claims the industry disputes. Medicare pays health plans higher rates for sicker patients but requires that the plans bill only for conditions that are properly documented in a patient’s medical records.
Researchers also have concluded that Medicare overpays the health plans by billions of dollars every year because of medical coding flaws that generate higher bills than are justified.
The whistleblower suits, mostly filed by former employees of healthcare companies, have long served as the primary tool for clawing back alleged overpayments. In January, Kaiser Permanente agreed to pay $556 million to settle Justice Department allegations that it billed the government for medical conditions patients didn’t have, the largest such penalty to date. In a statement posted on its website, the company said it settled the case “to avoid the delay, uncertainty, and cost of prolonged litigation.”
By contrast, CMS’ efforts to prevent Medicare Advantage plans from overcharging have largely foundered.
In 2014, for instance, CMS backed off a proposed regulation that would have cracked down on overbilling amid an “uproar” of opposition from the industry. And even when CMS audits uncovered tens of millions of dollars in overpayments, agency officials collected only a tiny fraction of that amount.
The CMS threat to bar Elevance from enrolling new members may open a new approach.
“The payment Elevance is making here is not trivial,” said Matthew Fiedler, a health policy researcher at the Brookings Institution.
But he noted that it represents a very small fraction of the total the company receives from Medicare. He said that making a big dent in the overpayment problem would require CMS to collect “many similar payments” — from “every” Medicare Advantage insurer.
“I don’t think there’s a clear reason to believe that at this stage,” Fiedler said.
Richard Kronick, a former federal health policy official and a professor at the University of California-San Diego, agreed that the payment reflects a small portion of the company’s revenue. But he said it was “still a sizable check to write.”
Kronick said the action reflects “perhaps a bit of muscle flexing” by CMS to tighten up enforcement.
CMS did not immediately respond to a request for comment. It’s not clear from court records whether the payment will end the CMS threat to ban Elevance from signing up new members.
If so, it might prove to be a relative bargain. In an April filing with the Securities and Exchange Commission, the company noted that its “current best estimate” of the “potential exposure” in the case was approximately $935 million.
Elevance has been at odds with the federal government over its billing practices since 2020, when the Justice Department filed a False Claims Act lawsuit against the company, then known as Anthem. That case is pending.
Court filings in that case disclosed the company’s payment to CMS. In an email made part of the court file, a company official confirmed it had sent the wire transfer in the amount of $342,209,085.30 on May 27 and said the payment was related to the threatened enrollment ban. The company also stated that it was challenging the CMS enforcement action and called it “unprecedented.”
In defending against the Justice Department suit, Elevance has denied wrongdoing and argued that CMS knew about its billing practices for years and took no action.
Meyers, the Brown University professor, said CMS’ success in collecting payment from Elevance may encourage more enforcement.
“It remains to be seen whether this is a sea change,” he said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Julie Rovner
KFF Health News
@jrovner
@julierovner.bsky.social
Read Julie's stories.
Julie Rovner is chief Washington correspondent and host of KFF Health News’ weekly health policy news podcast, "What the Health?" A noted expert on health policy issues, Julie is the author of the critically praised reference book "Health Care Politics and Policy A to Z," now in its third edition.
For the second year in a row, Trump administration officials are delaying the distribution of hundreds of millions of dollars in health-related grant funding as political appointees seek to ensure the funding adheres to the administration’s priorities — despite promises to Congress that the money would be spent as directed.
Meanwhile, four years after the Supreme Court overturned the federal right to abortion, nearly half the states have banned or substantially restricted the procedure. But while most voters say they support abortion rights — and majorities in several states have approved ballot measures to enshrine them — that sentiment has not translated into major gains for Democrats running for office.
This week’s panelists are Julie Rovner of KFF Health News, Maya Goldman of Axios, Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico Magazine, and Rachana Pradhan of KFF Health News.
Federal funding for health grants and international humanitarian aid is not reaching its recipients, demonstrating that congressionally authorized and appropriated funding is still encountering roadblocks under the Trump administration. At least some of the money is being tied up in review, with political appointees requiring personal signoff on any and all disbursements. While many lawmakers have made their frustrations known, Congress has few levers to ensure the money goes where lawmakers say it should.
This week marked the fourth anniversary of the Supreme Court case that overturned the constitutional right to an abortion. Yet research shows there were more abortions performed in the U.S. last year than there were in the year before the court’s decision. Access to medication abortion and telehealth prescribing are credited for that increase — two methods that activists who oppose abortion have targeted in their continuing efforts to eliminate it.
In vaccine policy news, a study showing the effectiveness of the covid vaccine that was spiked by Trump administration officials was recently published in a peer-reviewed medical journal. And Defense Secretary Pete Hegseth reinstated a flu vaccine mandate for the military after a significant flu outbreak at Lackland Air Force Base in Texas.
Amid concerns over healthcare affordability, two states are taking measures to address prices. A new Indiana law imposes price controls on hospitals, and Colorado has received federal approval to import drugs from Canada — though Canadian distributors have shown no interest in working with American states.
Plus, for “extra credit” the panelists suggest health policy stories they read this week that they think you should read, too:
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
Sen. Ron Wyden and 14 Democratic co-sponsors plan to introduce legislation Thursday to cap consumers’ potential out-of-pocket costs in traditional Medicare, resurfacing a long-running debate over why the program doesn’t limit beneficiary spending.
Even the bill’s backers say securing passage this year is a long shot. But the effort is one more opportunity for Democrats to highlight voters’ frustration about healthcare costs leading into the November election.
Polls show Americans are very concerned about affordability, with a recent Gallup survey finding fewer than half of Americans say they can consistently afford healthcare.
Wyden’s bill would focus on what many consider a critical pocketbook issue in traditional Medicare: There’s no limit on what a beneficiary could pay in cost sharing.
“Everyone else in the health insurance neighborhood has one — employer coverage, the Affordable Care Act, all of them have a cap,” the Oregon Democrat told KFF Health News. “There’s no good, common-sense reason why the flagship health program doesn’t have the same protection.”
Critics of a cap, meanwhile, are likely to pounce on the cost to the federal budget, which could be significant.
Wyden, already making the battle lines clear, added, “I suspect it will come up on the floor of the Senate that Democrats want to give a fair shake to people on traditional Medicare and Republicans want to help billionaires.”
Policy, Political Dynamics at Work
The underlying issue is the 20% share of Medicare costs that enrollees have to pay for medical services after they’ve met any deductibles. Without a ceiling or upper limit, an expensive condition such as cancer or a long hospital stay could result in beneficiaries paying thousands of dollars in costs.
That concern leads about 43% of people enrolled in traditional Medicare to purchase separate insurance, often called Medigap. (Others get such coverage through job-based retiree plans.)
Medigap insurance plans have seen rapid premium increases and can cost thousands of dollars a year, especially for couples. That price tag can be unaffordable for some beneficiaries, who may instead turn to private-sector Medicare Advantage plans offered by commercial insurers, or go without.
The Wyden proposal would set a $5,000 cap in traditional Medicare. Any amounts paid by a Medigap plan or a retiree health plan toward beneficiaries’ care would count toward that cap. It also includes other provisions to help older people with lower incomes, including eliminating an asset test to qualify for special programs that help reduce costs.
Medicare would pick up any amounts over that $5,000 limit, which is lower than the one Congress set for the rival Advantage plans — currently $9,250, although insurers can set smaller amounts.
Setting a cap in the traditional program, proponents argue, would help level the playing field between traditional Medicare and Advantage plans, which often cost consumers far less than traditional Medicare with a Medigap supplement. Premiums for these policies would probably be lower, they say, because the insurers’ financial exposure would be limited.
The Medicare Advantage program has historically had strong support from Republicans, who like its private-sector aspect and note that it can potentially do more to control costs, such as by using specific networks of doctors and hospitals, or requiring preapproval for some services, which the traditional program cannot do.
The plans also offer enrollees additional benefits, such as eyeglasses, hearing aids, and prescription drug coverage, and have now attracted more than half of all Medicare enrollees.
The bill has not yet been analyzed by the Congressional Budget Office, so there is no official estimate of increased costs to taxpayers for Medicare. Still, it would raise those costs — at a time when other health programs are being cut, the Medicare trust fund is scheduled to start falling short of funding in 2033, and the nation’s debt is growing.
That is likely to draw sharp rebukes from fiscal hawks and other conservatives who question whether billions in tax dollars should be used to pick up costs that would otherwise be paid by enrollees or by the supplemental insurance plans many purchase to do so. They are likely to note that beneficiaries could also choose to join private sector Advantage plans, which eliminate the need for supplementary insurance coverage such as Medigap.
Key Questions: Who Benefits? Who Pays?
A cap’s cost to taxpayers, while not officially scored yet, is likely to be significant, although adding one could also save individual consumers money. A recent study from Brown University gives some clues.
A $5,000 cap could save enrollees an average of about $1,200 a year, the study says, both in direct savings and reductions in their Medigap supplemental premiums. Just over 11% of traditional Medicare beneficiaries, about 3.2 million, would directly benefit from such a cap if it was implemented in 2028, said the study, which did not receive outside funding.
Over the next 10 years, it estimates, just over 52% of all traditional beneficiaries would exceed the $5,000 cap at least once.
Still, lead author Andrew Ryan, a professor at Brown’s School of Public Health, said analysts estimated such a cap “could cost over $50 billion annually, which is a lot of money” to add to the federal balance sheet.
Critics are likely to focus on the cap’s expense and the number of people who might benefit.
“How many people are hitting a level of cost they can’t afford on Medicare? “asked Jackson Hammond, a senior policy analyst with the Paragon Health Institute, a conservative think tank influential with the GOP.
Any cap “is generally going to increase expenses for the program without adding a lot of benefits to enrollees,” said Hammond, who spoke with KFF Health News before the legislation was introduced.
Supporters, though, have a different view.
Certainly, with “any policy that’s going to cost money, there will be an argument over where the money is coming from,” said Brian Keyser, a research associate at the liberal Center for American Progress who also spoke with KFF Health News before the Wyden measure was introduced.
Keyser co-authored a Medicare paper that suggested lawmakers could pay for changes in traditional Medicare, such as an out-of-pocket cap, if they reduced the amount the government pays Medicare Advantage insurers, pointing to government estimates that Advantage would cost the government $76 billion more this year than if the same number of people were in the traditional program.
Finding a way to add a cap “is right and fair because without it, people who become seriously ill can spend their life savings on cost-sharing Medicare,” Keyser said.
Such an idea, however, has been in discussion on and off for years. Knowing that, the bill’s backers acknowledge that passage is unlikely — but they say they’re playing the long game for now.
“We’re going to push for it in the next Congress, when we believe we will be in the majority,” Wyden said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
One afternoon in late 2024, a sixth-grader nicknamed Bug came home from school with an announcement to make. Bug, who was assigned female at birth, told his parents he was a boy — and would be using he/him pronouns.
“OK, cool,” his mother, J, remembered saying. (J asked to be identified by only her first initial, and Bug by his nickname, because the family fears harassment.)
“‘What do you need to be supported?’” she recalled asking next. “He asked to get healthcare.”
This was the kind of moment J had been anticipating since the family had moved earlier that year from Texas to Massachusetts, for its more liberal and inclusive politics. She felt confident they could find the right medical experts. But she hadn’t realized that access to gender-affirming treatment could disappear even when their state’s laws and leaders supported it.
Individual hospitals all over the U.S., in red and blue states, have responded to President Donald Trump’s attacks on transgender healthcare by deciding to withdraw care on their own. At least 20 hospitals did so in the first months of the Trump administration as it threatened to pull back federal funding or initiate fraud or wrongful-claim investigations, and such services have continued to drop off since.
Bug and his younger sister were born in Austin, Texas, but J and her husband became worried after the state outlawed abortion; dismantled diversity, equity, and inclusion programs; and limited medical and civil rights for queer and transgender people. The parents worried the support services they needed for the siblings, both of whom have autism, might be affected, too.
“I had a fear of being like the frog in the boiling water and not realizing what was happening until it was too late,” J said. “I needed to get the kids out of Texas.”
After Bug’s gender announcement, J’s queries led her to the largest hospital system in the region, Springfield, Massachusetts-based Baystate Health, where they began the months-long process of getting set up to start hormone therapy.
Bug, an artistic 14-year-old who loves horses, cats, and making short films with friends, was too old for puberty blockers, but he was excited about the prospect of starting on testosterone. That would cause his voice to deepen, facial hair to grow, and muscles to get bigger.
“Every part of it sounds fun,” he said.
J (right) and her son, Bug, at their home in western Massachusetts. Bug, who came out as a trans boy in 2024, had turned to Baystate Health for treatment until the health system stopped providing gender-affirming medications to youths. (Karen Brown/New England Public Media)
But this past February, two weeks before Bug was scheduled to start testosterone, Baystate announced it would no longer provide gender-affirming medications to minors, offering only counseling. A letter to patients’ families did not explain why.
Baystate spokesperson Heather Duggan sent a statement that said the decision to end treatment for minors reflected the fact that Baystate could lose “hundreds of millions of dollars in government reimbursement” as a result of the Trump administration’s plans. “Nearly 70 percent of Baystate Health’s patients rely on Medicaid and Medicare for coverage,” it said.
All Bug knew was that the care he’d eagerly awaited was about to vanish.
“I felt frustrated that they would do that,” Bug said.
“I bet there’s tons and tons of kids who are like: ‘OK, I’m going for trans-affirming healthcare. Yay!’” he said. “And then, like, tons and tons of kids were disappointed and sad and frustrated.”
J said it felt as if the floor had fallen out from under them. “Maybe this is naive, but I didn’t think that would happen in Massachusetts,” she said.
Baystate is among the providers still choosing not to offer puberty blockers and hormones as the issue wends its way through the courts. This spring, in a lawsuit that Massachusetts joined, a federal judge concluded that it was unlawful for the Department of Health and Human Services to threaten federal funding for providers that offered gender-affirming care to minors. In June, another federal judge cleared 16 states, including Massachusetts, to move forward with another lawsuit against the administration over its push to criminalize gender-affirming care.
Baystate Medical Center in Springfield, Massachusetts. The Baystate Health system stopped providing gender-affirming medications to youths in February, after the Trump administration said it would pull Medicaid and Medicare funding from hospitals providing them. (Karen Brown/New England Public Media)
The American Academy of Pediatrics declined an interview request but said in a past statement that young patients and their families should make decisions about gender-affirming care with their doctors, “delivered with compassion, and offered without political interference.”
One mother of a former Baystate patient said that before her child came out as a transgender girl, she had been severely depressed, battling suicidal thoughts. (The mother asked that only her first initial, L, be used, because the family also fears harassment.)
After Baystate doctors prescribed puberty blockers and estrogen, her daughter’s mood and grades rose markedly, L said. So when she received the letter announcing Baystate was ending the medical treatment, she was furious. L said she and other parents filed civil rights complaints with the Massachusetts attorney general.
The attorney general’s office did not respond to a request for comment.
“There’s a sense of, ‘How could you?’” L said. “And there’s also the awareness of the impact just pulling care could have on a youth — from a physical health perspective but also from a mental health perspective.”
L and J both found alternatives for their children. L asked the family’s primary care doctor to take over hormone prescriptions. Bug’s family was referred to Transhealth, a private specialty clinic in Northampton, Massachusetts, that said it has taken on about 50 of Baystate’s former patients.
“Transhealth has been staffing ourselves up for a while now in anticipation of the fact that this may be happening across the state,” CEO Jo Erwin said.
Erwin said Transhealth can weather the funding threats because the clinic gets large private donations and is not as dependent on Medicaid and Medicare as most hospitals. But Erwin said that doesn’t entirely reassure the broader LGBTQ+ community, including transgender adults.
“When you see something like that go down, people get scared that it’s ultimately going to happen to everyone,” Erwin said.
In May, Colorado’s Supreme Court ordered a children’s hospital in that state to resume medical treatments for transgender youths, while in Texas a court settlement compelled a children’s hospital there to do the opposite — start the nation’s first “detransition clinic.” The Trump administration has continued to pressure providers, including by seeking the medical records of transgender minors.
After Bug’s false start at Baystate, he was able to start taking testosterone at the new clinic in the spring.
His mother, J, said that the treatment is going smoothly and that Bug has learned how to give himself the injections. But J is nervous that the federal government will find other ways to stop his treatment again. She sometimes second-guesses the family’s move from Texas to Massachusetts, wondering whether they should have gone to Canada instead.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.

















{kind=link}