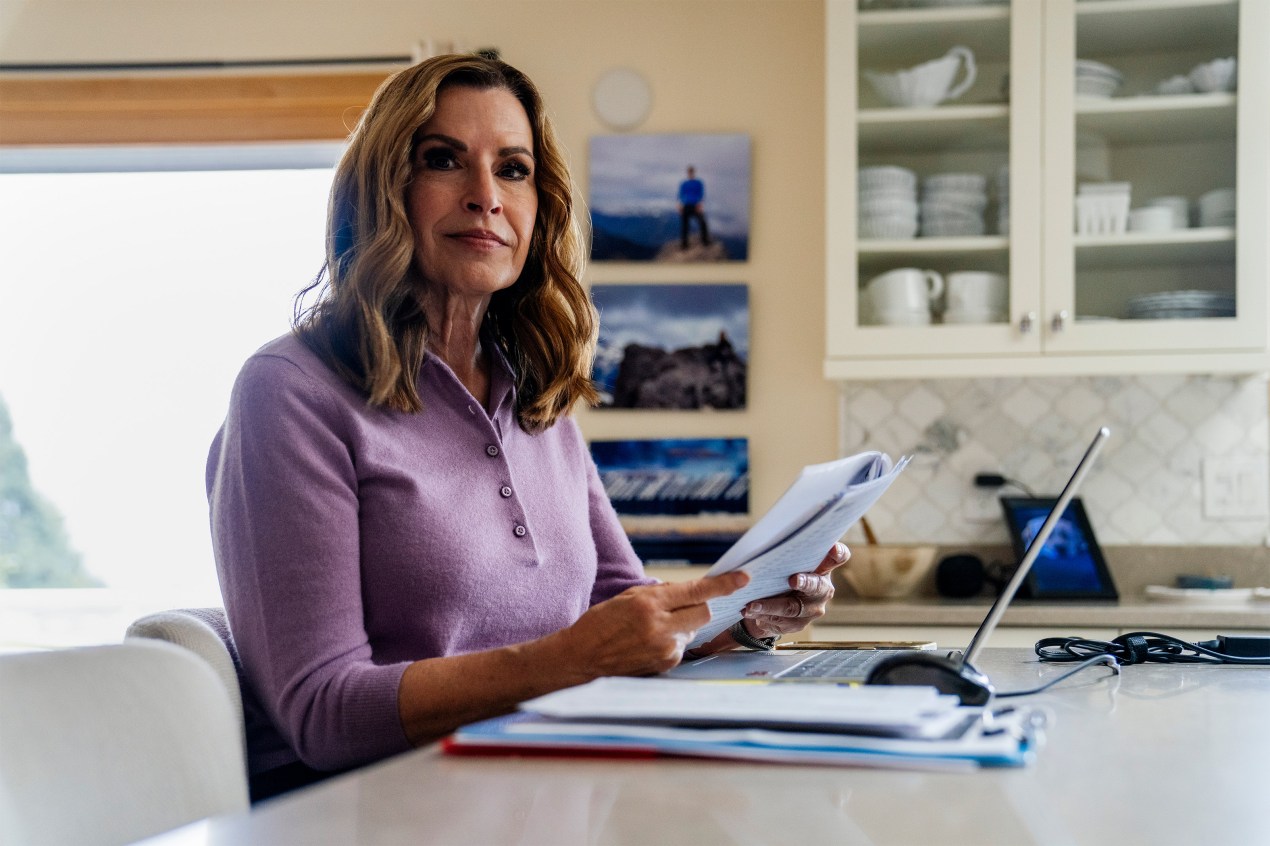
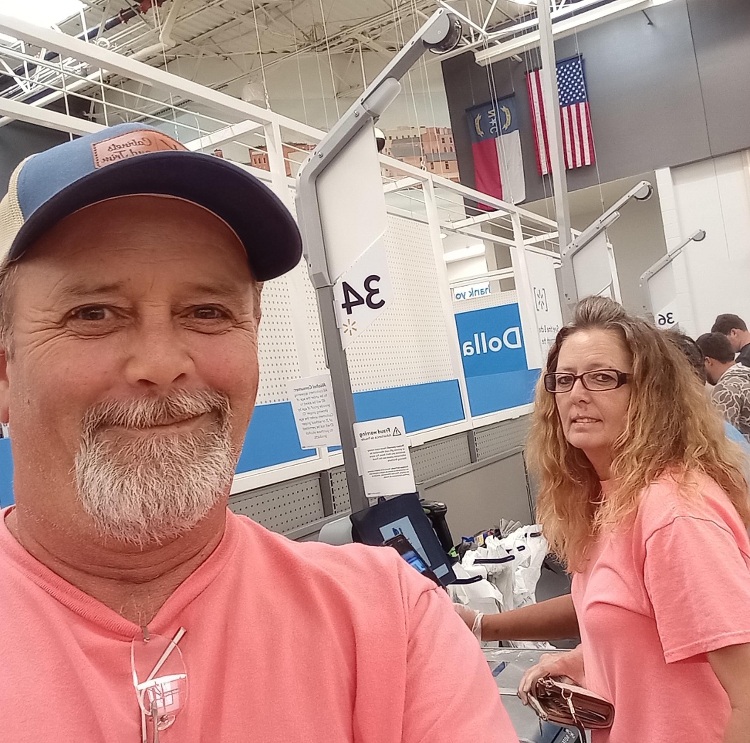
On April 10, 2025, several hours after finishing a hike in Sedona, Arizona, Jan Anderson started repeating herself.
“Did we hike this morning?” she asked.
“Yes, we hiked,” said her husband, Steve Francks. “And you did really well.”
But 15 seconds later, she asked the same question: “Did we hike today?”
Anderson, 65, a retired finance executive, doesn’t remember any of it. She can recall what happened that afternoon only because her husband started recording her on his cellphone.
“I was just on this nonstop loop,” she said.
Almost immediately, Francks knew something was wrong. “Jan was out of it,” he said.
He took her to an emergency room in Sedona, where staff initially thought she might be having a stroke. Because the facility wasn’t fully equipped to evaluate or treat stroke patients, Francks said, she was airlifted to a Phoenix-area hospital, where she was admitted.
It turned out she wasn’t having a stroke. Her medical team eventually determined she was probably experiencing transient global amnesia, a rare, temporary, and benign memory disorder.
The good news was that her symptoms didn’t last long, and she has suffered no long-term effects from the episode. It took about 24 hours before she was able to start forming new memories, and she was discharged the next day. Anderson and Francks, who split their time between Sedona and Edmonds, Washington, returned to the Pacific Northwest a few weeks later.
Then the bill came.
The Medical Service
The sudden confusion associated with transient global amnesia can also be a sign of a more common neurological condition, so it’s important to rule out other possible causes — such as a stroke, for which timely emergency care can spell the difference between life and death.
Anderson’s records show her care at Abrazo Health’s Arrowhead Campus in Glendale, Arizona, included an electrocardiogram, which can detect underlying cardiac abnormalities, and imaging, which would rule out any vessel blockages that might cause a stroke. She also underwent various lab tests commonly used to diagnose a stroke.
The Bill
$59,181: $35,302 for diagnostic/therapeutic imaging, $8,147 for laboratory services, $8,146 for a special care unit, $5,532 for EKG services, and $2,054 for pharmacy. Anderson’s first bill from Abrazo Health said she owed $15,312.43, citing an insurance adjustment of $43,868.57, even though her insurer had not covered any of the charges.
Anderson said her insurer covered separate charges for the ER and helicopter transfer.
The Billing Problem: Communication Breakdown
The federal No Surprises Act bans out-of-network bills for most emergency services, even if those services are received at an out-of-network facility and are not preapproved by the insurer.
That means the cost of Anderson’s hospital care should have been covered as though it were in-network. At the time, she was insured by Molina Healthcare, through a plan purchased on the federal Affordable Care Act marketplace.
But for a year, Molina declined to pay for her care in Glendale, at one point arguing that her hospital stay required authorization when, or even before, she was admitted.
“I can’t get anyone to resolve it,” Anderson said. “It’s almost $60,000 hanging over my head.”
The first problem arose about two weeks after she was discharged, when Abrazo Health sent Anderson a bill indicating she was a self-pay patient.
The hospital didn’t request her insurance information at any point during her stay, Francks said. He assumed, at the time, that his wife’s financial paperwork had been transferred from the ER in Sedona. It had not.
She called the Glendale hospital and corrected the error.
Then, in late June, Anderson received notice from the hospital indicating she was not a Molina member.
“Your insurance company notified our office that the patient was not a covered member for the services provided by Abrazo Arrowhead Campus on the above referenced service date(s),” the notice said. It showed the total charges for her stay exceeded $59,000.
But when Anderson called Molina to confirm her coverage, she said, the insurance company assured her the claim was being processed.
That didn’t mean Molina was willing to cover her hospital bill.
Anderson spent months trying to resolve the balance. She filed complaints with members of Congress, the Arizona Department of Insurance and Financial Institutions, and the Office of the Insurance Commissioner in Washington state.
In an October letter to Washington’s insurance commissioner, an appeal and grievance specialist for Molina wrote that the claim was denied because “inpatient stays require prior authorization, or notification at the time of admission. No notification of admission or prior authorization was received from the hospital, so the claim was denied.”
It continued: “Molina covers out of network emergency services but since this was an inpatient admission authorization is required.”
Nicole Broadhurst, who focuses on medical billing issues as CEO of a Tennessee patient advocacy group, said this dispute appears to rest between the insurer and the medical provider.
She said that Anderson’s insurance information should have been transferred between the first ER and the Glendale hospital. Since it wasn’t, Broadhurst said, Anderson shouldn’t be held liable for her hospital bill. (Broadhurst was not involved in efforts to resolve Anderson’s billing dispute.)
Unfortunately, Broadhurst said, these situations are “not uncommon, even though we have the No Surprises Act.”
The Resolution
Anderson said she was told by Abrazo Health for months that it was working with Molina to resolve the bill. She said she was also told that even if Molina did not cover the full cost of her hospital care, she would not be liable for the balance — but she never received that assurance in writing.
Meanwhile, Molina continued to uphold its decision to deny payment.
After KFF Health News contacted the insurer and the hospital with questions about her case, Molina told Anderson it had launched an internal review of her claim, and a revenue director with Abrazo Health told her the company was “treating this as a high-priority matter,” she recalled.
Anderson said the revenue director for the health system assured her that if Molina continued to deny payment, “the balance will be written off on the hospital’s end,” she said. “I will not be responsible for any balance” — not even the $15,312.43 the hospital initially billed her after the hospitalization.
Linda Nofer, a spokesperson for Abrazo Health, would not answer questions about Anderson’s bill. In a statement, she said the hospital system is “committed to working closely with our patients to resolve billing questions and concerns.”
Molina spokesperson Caroline Zubieta would not discuss or respond to questions about Anderson’s case on the record.
The Takeaway
The flurry of insurance paperwork and medical bills patients receive after a hospital stay can be overwhelming — and may sometimes appear contradictory.
Broadhurst said it’s important for patients to focus on the “patient responsibility” portion of an insurance document called an explanation of benefits.
Patients should not pay a bill if their explanation of benefits indicates they aren’t responsible for the amount charged.
In this case, Anderson had received a bill from the hospital saying she owed money. And her explanation of benefits from Molina confirmed she’d racked up more than $59,000 in hospital charges.
But that document also indicated her patient liability was “$0.00.” Anderson said the hospital was not pressuring her to pay the $15,312.43 bill or any of the charges tied to her account, but she was worried she would eventually owe a large sum because the charges remained unresolved for more than a year.
“The question I kept asking them was, ‘How much am I going to owe?’” said Anderson, who is now insured by Medicare. “It could be anywhere from that $15,000 adjusted amount to the full balance of $59,000.”
Broadhurst said she tells patients facing similar situations to “send the hospital a copy of the EOB and ask them to correct the account to $0 patient responsibility.”
“Even if no one is actively trying to collect, I’d still push for written closure so it doesn’t keep hanging over them,” she said.

Bill of the Month is a crowdsourced investigation by KFF Health News and The Washington Post’s Well+Being that dissects and explains medical bills. Since 2018, this series has helped many patients and readers get their medical bills reduced, and it has been cited in statehouses, at the U.S. Capitol, and at the White House. Do you have a confusing or outrageous medical bill you want to share? Tell us about it!
This <a target="_blank" href="https://kffhealthnews.org/health-care-costs/amnesia-arizona-hospital-prior-authorization-bill-of-the-month-may-2026/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2241524&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">from Health Industry Archives - KFF Health News










{kind=link}