Prominent doctors at UVA Health System are expressing public outrage at their employer’s practices to collect unpaid medical debt from its patients.
A Kaiser Health News report in September that showed UVA sued 36,000 patients over six years for more than $100 million, seizing wages and savings and even pushing families into bankruptcy.
Like many physicians who work at U.S. medical centers, the UVA doctors said they had little idea how aggressively the hospital where they practice was billing and pursuing their patients for payment.
Although the health system has announced some interim measures to scale back collections practices, some of the system’s most senior physicians are now calling for UVA to stop suing its patients altogether. And they are urging the pursuit of an “immediate solution” to address the national epidemic of health care debt.
“We were appalled by the revelations of the aggressive, pitiless billing and collections practices” at UVA, Dr. Scott Heysell and two other senior staff members wrote in a letter to KHN published Saturday. “We felt betrayed,” they wrote, “and we had, by extension, betrayed those who had relied on us.”
Heysell, an infectious-disease specialist and associate professor at UVA School of Medicine, and his co-authors echoed other UVA researchers and clinicians contacted by a reporter who said they were surprised and dismayed by the health system’s practices.
UVA initially defended its practices, pointing to the Virginia Debt Collection Act of 1988, which requires state agencies to “aggressively collect” money owed. But within days of the KHN report, UVA said it would reduce its use of the courts and make it easier for patients to qualify for financial assistance.
That’s not enough, said the letter’s authors, who include Dr. Rebecca Dillingham, director of UVA’s Center for Global Health, and Dr. Michael Williams, director of the UVA Center for Health Policy.
They ask “why UVA cannot join other public hospitals that have effectively stopped suing patients altogether?”
Other University of Virginia faculty said the system’s practices undermined their efforts to improve care for middle- and lower-income families and was not in keeping with an ethos of putting patients first.
KHN’s findings “made me feel utterly hypocritical about my work and efforts to promote health equity,” Rajesh Balkrishnan, a UVA public health professor who researches cancer treatment in Appalachia, said in an interview.
“This is a public university with one of the richest endowments in the country,” he said. At least take care of the immediate community you serve.”
In September, UVA Health said it would “reduce our reliance on the legal system,” suing patients only if their household income is more than 400% of the federal poverty level, or $103,000 for a family of four. It also pledged to increase discounts for the uninsured and upgrade its financial assistance for patients.
Those measures are “a first step,” it said. On Oct. 28, it named an advisory council of community leaders, patient advocates and UVA students and staff to consider further changes.
“We are continuing to thoughtfully review our billing and collection practices to find additional ways to better serve our patient as well as improve fairness and transparency,” said UVA Health spokesman Eric Swensen. “We are looking at all options to achieve these goals.”
Virginia Gov. Ralph Northam, who oversees the state’s university system and public hospitals, is a pediatric neurologist.
“As a doctor himself, Gov. Northam agrees with the doctors who have taken a stand against unfair and aggressive medical billing practices,” his spokeswoman said. “Much more can and should be done to address this issue.”
KHN’s report prompted discussions across the campus in Charlottesville about how to treat uninsured patients or those with coverage who still struggle with thousands of dollars in out-of-pocket expenses, doctors and faculty said.
“No physician wants to be responsible for bankrupting a patient — not one physician, not one patient,” said Dr. Mohan Nadkarni, UVA’s chief of general internal medicine. He is the only physician on the advisory council.
“UVA physicians were completely taken aback by the scale and magnitude of the collections practices,” Nadkarni said. Discussion at the council’s first meeting reflected “lots of pent-up dissatisfaction from community leaders” about UVA’s practices, he said.
But many knew the health system was suing patients, they said. Some had firsthand experience with aggressive tactics from the billing office.
At one “town meeting” of health system employees, held at UVA’s Leonard Sandridge Auditorium in response to KHN’s report, somebody took the mic and asked, “Who in this room has been taken to collections by UVA?” said Matthew Gillikin, a speech therapist who was there. A third to half the people raised their hands, he said.
Court data analyzed by KHN showed that UVA Health was suing about 100 of its employees every year.
Also at the town meetings, “we heard many agonizing stories of patients and employees having been sued or having wages garnished,” Nadkarni said. “We heard loud and clear from many physicians that they heavily supported significant liberalization” of UVA Health’s financial assistance policies.
Family physician Dr. Alex Salomon, who worked at UVA for seven years and now is with Augusta Health in Fishersville, Va., had “a lot of patients” with UVA bill and lawsuit problems, many who had insurance but could not make out-of-pocket payments, he said. Still, he added, “I didn’t realize UVA was so much worse” than other hospitals.
As part of the University of Virginia, UVA Health is a state institution that is not subject to taxation. UVA Medical Center, the system’s flagship hospital, made a $91 million operating profit on revenue of $1.8 billion in the fiscal year ending in June and held stocks, bonds and other investments worth about $1 billion.
Doctors are realizing that financial barriers to treatment and budget squeezes from bills can be as harmful to patients as disease, said Dr. Marty Makary, a surgeon and researcher at Johns Hopkins Medicine who studies hospital debt collection and is urging UVA alumni to press for further change.
“I have not talked to a single patient or student of UVA or faculty member or alumni who thinks it is reasonable for the hospital to sue patients who cannot afford their bill,” he said.
News of UVA collections practices served as a teaching moment for at least one class.
“Many of the students in my class work for the UVA Health System, so the recent media coverage about UVA’s billing practices has been painful for them as nurses who care deeply about the patients and families they serve,” Kimberly Acquaviva, a professor who teaches health policy at UVA’s nursing school, tweeted in September. “As a class, we talked about the power that nurses have to shape the lives of the patients and families” by advocating for system change, she said.
She declined a request for an interview, as did five other doctors or professors. Several referred a reporter to UVA spokesman Swensen. About 20 others did not respond to interview requests.
Dr. Chris Ghaemmaghami, an emergency and internal medicine doctor, became UVA Health’s acting CEO after Pamela Sutton-Wallace announced her resignation in September. Her departure was unrelated to KHN’s revelations, UVA said at the time.
“I understand the disappointment some fellow physicians felt when our historic billing and collection practices came to light,” he said in an email responding to questions from KHN.
Heysell, Williams and Dillingham, the doctors who wrote the letter, go further.
“To be clear, we are outraged,” they write. “We stand with those that have been financially injured, whose bank accounts have been looted, whose homes have been swallowed as if they were built on quicksand, whose credit scores were ruined, and whose mental health and energy were spent in a courtroom or in anxious conversations with lawyers — all as a result of having sought our care.”
Letters to the Editor is a periodic feature. We welcome all comments and will publish a selection. We edit for length and clarity and require full names.
First Do No Harm: When Financing Health Care Becomes Unethical
We attribute the oldest text of ethics in Western medical practice to Hippocrates (460-370 A.D.), a Greek physician whose oath instructs, “I will use treatment to help the sick according to my ability and judgment, but never with a view to injury and wrong-doing.” Most doctors, having pledged that oath upon entering the profession, recall best its later paraphrasing primum non nocere, first do no harm.
As physicians at UVA Health and educators at the University of Virginia, we were appalled by the revelations of the aggressive, pitiless billing and collections practices, first reported in The Washington Post based on an investigation by Kaiser Health News (“‘UVA Has Ruined Us’: Health System Sues Thousands Of Patients, Seizing Paychecks And Claiming Homes,” Sept. 10). We felt betrayed and we had, by extension, betrayed those who had relied on us. We had harmed.
When we began our positions at UVA, we did so with the understanding that, as clinicians at a public institution, we were privileged to care for all people, including those with limited ability to pay. Many of us chose academic medicine, and UVA specifically, so that we could partner with our patients to improve health and well-being thanks to the social contract specific to tax-exempt hospitals to provide low-cost care to people of all incomes. As we have learned recently about UVA and from stories reported from other states and institutions for more than a decade, avaricious billing and collections practices have broken the spirit, if not the letter, of that social contract (“UVA Doctors Decry Aggressive Billing Practices By Their Own Hospital,” Nov. 23).
The individual stories are heart-rending, and the extent of the collective impact is staggering. Indeed, based on an analysis by the Consumer Financial Protection Bureau in 2014, over half of all collections items in credit reports are associated with medical debt. A recent study of people with new diagnoses of cancer and a representative insurance mix, including the uniquely American categorization of people underinsured, found 42% had depleted their life savings 2½ years after their diagnosis. To be sure, academic medical centers must function within the competitive and revenue-driven environment of our country’s approach to health care, and some, like Hahnemann Hospital in Pennsylvania, have not survived. However, the survival of not-for-profit hospitals cannot be assured by the relentless pursuit of debt from the very patients for whom we are expected to be the safety net.
Senate Finance Committee Chairman Chuck Grassley (R-Iowa) sent a letter on Oct. 17 to the UVA Health System’s acting executive vice president for Health Affairs that detailed questions about billing and collections practices at our institution. We have similar questions. While we applaud UVA for the rapidity with which it has announced reforms aimed at reducing the numbers of lawsuits and making more financial support available, we are uncertain how many future lawsuits will be prevented by restricting that punitive action to those with bills of more than $1,000, and why UVA cannot join other public hospitals that have effectively stopped suing patients altogether?
We simply cannot accept one-off solutions. Over half of all hospitals in the U.S. are not-for-profits, and the regulations that govern billing and collections practices vary by state and fail to offer adequate protection in most. Continued identification of egregious practices at individual institutions is essential, and we are grateful for the work of health care journalists and of members of Congress who have prioritized these issues in the national discourse. Public pressure placed on hospitals has frequently resulted in forgiveness of debt and, in some cases, changes in billing practices. Yet, until we achieve a truly universal health system modeled after other countries with similarly vast monetary wealth but more concrete social moorings, we must pursue an immediate solution to address health care pricing and billing. Such a solution must ensure transparency, as Sen. Grassley rightly highlights in his requests of UVA, and therefore allows for honest conversations about how we, as a country, hope to continue to provide excellent care to all Americans. The National Consumer Law Center’s Model Medical Debt Protection Act could serve as an important starting point.
To be clear, we are outraged. We stand with those that have been financially injured, whose bank accounts have been looted, whose homes have been swallowed as if they were built on quicksand, whose credit scores were ruined and whose mental health and energy were spent in a courtroom or in anxious conversations with lawyers — all as a result of having sought our care. We commit to working at UVA, our beloved professional home, to advocate for leaders of high moral integrity, to regain the trust of our patients and to repair to the greatest extent possible the damage that has been done. We call on our community, and especially our fellow clinicians, to demand that the precious resource of our public, not-for-profit hospitals protect our ethical responsibility to first do no harm.
— Drs. Scott K. Heysell, Michael D. Williams and Rebecca A. Dillingham, University of Virginia, Charlottesville, Va.
It’s good news that predatory hospital billing and collection practices are being questioned (this time at a location we get care from): https://t.co/rT2MlRdnZo
Fears over patient falls are warranted; however, steps should be taken to provide patients with access to physical therapy while in the hospital to prevent loss of strength and mobility. Further, access to physical therapy can help reduce the steep costs associated with falls, which total roughly $50 billion annually.
In the outpatient setting, physical therapists are uniquely qualified to improve a patient’s functional ability and recommend the home modifications necessary to allow them to remain independent.
Whether inside the hospital or in the outpatient setting, patients need to be allowed and encouraged to move and walk under the supervision of a physical therapist. Promoting access to physical therapy will ultimately keep our seniors independent, prevent adverse events and drive down health care costs.
― Nikesh Patel, PT, DPT, executive director of the Alliance for Physical Therapy Quality & Innovation, Washington, D.C.
Another poorly thought through CMS regulation. Quality healthcare cannot be reduced to yes or no questions. ‘Fear Of Falling’: How Hospitals Do Even More Harm By Keeping Patients In Bed https://t.co/GTO1xLTDU6 via @khnews
I’ve been a Kaiser Permanente psychologist for over 25 years. I have seen many changes with Kaiser and I am tired of having to shortchange my patients of much-needed treatment services (“Bruising Labor Battles Put Kaiser Permanente’s Reputation On The Line,” Nov. 8). I wrote this song on behalf of my therapist colleagues in protest for better working conditions for patient care in the Department of Psychiatry at Kaiser. I recorded it with another colleague, Matt Torres, and two musician friends who are Kaiser members and sympathetic to the NUHW cause.
The police in this article said they need to know whether they’re dealing with a mental health issue or drugs in order to respond appropriately. In Substance Abuse and Mental Health Services Administration’s 2018 report “Key Substance Use and Mental Health Indicators in the United States,” the percentages of adults who used illicit drugs in the past year were higher among those with serious mental illness (49.4%) and adults with any mental illness (36.7%), compared with those without any mental illness (15.7%).
Since there is such a high chance that people with mental illness are also using substances that can alter their clinical presentation, the police should be trained to prepare for modalities that can accommodate that, keeping themselves and those they serve safe.
― Xi Lucy Shi, Pittsburgh
Standing By Drug Treatment For ADHD
I am a child psychiatrist with a research and clinical focus on treatment of attention deficit hyperactivity disorder. I recently submitted a grant to the National Institute of Mental Health examining the evidence for and against stimulant treatment. The individuals quoted in the article “Pediatricians Stand By Meds For ADHD, But Some Say Therapy Should Come First” (Sept. 30), arguing that behavioral interventions are effective enough to be considered the first choice in ADHD treatment, aren’t correct.
Repeated, large-scale, well-controlled double-blind studies have shown that, with the exception of preschool/kindergarten children: (1) Medication for ADHD is shown to be significantly more effective than behavioral interventions, with behavioral treatments for ADHD only mildly effective or not effective at all. (2) Medication improves long-term outcomes, such as reduction of motor vehicle accidents, accidental physical injury and delayed educational progression. (3) Untreated ADHD is associated with increases in suicide risk, legal issues, divorce rate, job loss, substance use, motor vehicle accidents and self-esteem issues.
While the 6-year-old child in this article has tantrums (which might improve with only behavioral interventions), a school-aged or older child with ADHD would have problems with attention and concentration in school ― hurting his/her early learning. Symptoms of attention and concentration are particularly poorly responsive to behavioral interventions.
Behavioral treatment is not the first choice because delaying treatment can quickly have consequences, while medication treatment is very low-risk, yet dramatically effective.
― Dr. Ryan S. Sultan, New York City
Modifying classroom instruction and using behavioral supports should be first. Then meds if they are needed at the lowest effective dose along with modification and behavioral support.
Jeez
Your recent story about the cost of air ambulance services (“Bill of the Month: The Air Ambulance Billed More Than His Surgeon Did For A Lung Transplant,” Nov. 6) failed to paint the full picture. Recently, my wife had a Type A aortic dissection. She was transported to emergency surgery via helicopter air ambulance for a six-hour-long heart operation that saved her life. Our bill for the air ambulance was over $81,000 for the hour-long flight. What I learned from this incident is that there are only four hospitals in all of California where this operation is performed. Without the air ambulance, I would have likely been planning a funeral instead of dealing with over $750,000 in medical bills. The highly trained crews of these operations save lives every day. Most fly a helicopter, which costs $6,000,000 before it is equipped as a flying ICU. Most fly between one and three flights in a 24-hour period, on average. They are manned 24/7, equipped to fly in the clouds and equipped with night-vision capability. Nearly all are single-pilot crews (to keep costs lower) and have at least one flight nurse (most have two). All have training and qualification maintenance costs for the equipment and personnel. In consideration of all of these costs (note: I did not include facility or insurance costs), I think their cost to the patient is not out of line with other medical costs today.
I noted there was no talk of using a ground ambulance in the article. Was it time-critical for the patient? In other words, would it have had a similar outcome if a ground ambulance been used? In our case, the two extra hours a ground ambulance would have consumed would have likely concluded in a fatality.
The other side of this conversation revolves around how patients are billed and how our current system works to be the most expensive system in the world with only mediocre results. Nearly all billing is reduced by some amount by the insurance ― often called a discount. Because doctors and hospitals know they will receive only between half and three-quarters of what they bill, they inflate the billing so they get what the need to cover most costs. The big loser is the patient, who is underinsured or not insured at all.
The article as written is a very incomplete picture of the air ambulance world and a disservice to your readers.
― Dennis Lyons, Paso Robles, Calif.
Just read your article about helicopter charges. Why not educate the public that they can purchase helicopter insurance, which is very cheap? I highly recommend it to friends who live in rural areas with hospitals that do not offer a full range of services or who need transportation to receive a higher level of trauma care. A bigger problem: the huge health care systems ― whether privately managed or government-run ― that have associates with these rural hospitals or own them. They want patients to stay in their system and will bypass other hospitals that are closer and offer the same services. Choices of care are not always given to patients, or when they are given, they are brief and come in a moment of crisis when patients and families can’t take it all in. How about educating the public on what really is happening and how we continue to waste health care dollars and how they can protect themselves in advance? Call the air transport company and learn about their insurance.
― Nina Jeffords,Miramar Beach, Fla.
The associated "fact sheet" was equally bizarre and rather incoherent..this is a far cry from the normal professional and policy-oriented communications we expect from HHS.
Shefali Luthra did an excellent point-for-point takedown of President Donald Trump’s speech at a conservative retirement community in Florida, which amounted to a cynical gambit of frightening Caucasian seniors into believing that their long-cherished Medicare was under attack from the Democratic “socialist” and the freeloading communities they represent (“KHN & PolitiFact HealthCheck: Trump Speech Offers Dizzying Preview Of His Health Care Campaign Strategy,” Oct. 3).
One critical point that she and others, including the Democratic candidates for president, however, have failed to give sufficient emphasis to, is the degree that household income will actually increase in response to a “Medicare for All” plan. Trump stated in this speech, with no evidence, that household income will go down $17,000 a year with Medicare for all. Although there will be a tax increase to fund this program, the increase will pale in comparison to what we are already paying in premiums and deductibles to a predatory insurance industry. Ms. Luthra only went so far as to question the accuracy of that absurd assertion. Failure to drive this point home will invariably allow the masses to revert to the default mode of “socialized equals a tax increase ― end of story,” and put its long-overdue implementation at risk.
― Samantha Derrick, Berkeley, Calif.
Good, in-story fact check.But could context that current efforts aimed at serious reducing protections through ACA and #GOP has never offered any legitimate alternative > Trump Speech Offers Dizzying Preview Of His Health Care Campaign Strategy https://t.co/8waboBoT1B via @khnews
Great story about a little-known expense patients have for compression garments (“Compression Garments Can Ease Lymphedema. Covering Costs? Not So Easy,” Oct. 23). I had to purchase some to wear for a short time for lupus-related swelling and I was shocked at how much they cost. They definitely make a big difference in comfort, and I really think insurers should pay. As they also help to prevent infection, it may make coverage cost-effective in the long run. Is there a petition I can sign to support legislation? I will call my Congress members as well. Thanks for the article!
― Kristan Thompson, Savannah, Ga.
Penalties Run Afoul
In response to Jordan Rau’s article on Medscape.com (“New Round of Medicare Readmission Penalties Hits 2,583 Hospitals,” Oct. 1): If the hospital does not want to be penalized for readmission, well, the hospital staff can just let the patient die. On the contrary, the hospital should be rewarded for saving the life of the patient, and that is all that should concern Medicare. The hospital should be penalized for any patient deaths, period! Because the way around that penalty from Medicare is to just let the patient die in the hospital. It should be that the hospital is recognized for giving treatment to the best quality care that the hospital can provide! Someone should look into Medicare’s revolting penalty system.
― Harold A. Maio, Fort Myers, Fla., former editor of Boston University’s Psychiatric Rehabilitation Journal
I had injured/panicked bipolar client strapped on board call me frm accident scene bc cops on the way. She was afraid they’d shoot her. I get there, find Fire Capt next 2 her ready 2 protect her. Taking The Cops Out Of Mental Health-Related 911 Rescues – https://t.co/6f7k9Ehdf7
According to the U.S. Department of Health and Human Services, 80 million Americans lack access to primary care, with the most significant shortages in rural areas. By 2030, the country is expected to face shortages of more than 120,000 primary care physicians.
The nation’s 270,000 nurse practitioners (NPs) can address the shortage. In fact, a study in Health Affairs found NPs now represent 1 out of 4 health care providers in rural health practices. NPs assess patients, order and interpret tests, develop treatment plans and prescribe medications in all 50 states ― yet outdated state laws stand in the way.
Forty percent of states authorize full practice authority (FPA) for NPs, ensuring patients full and direct access to NP care. The remaining states limit NPs from practicing to the top of their education and training.
NPs can meet the demand for high-quality primary care nationwide. It’s time the remaining states update their laws so that all patients can access the care they deserve.
― Sophia L. Thomas, president of the American Association of Nurse Practitioners, Austin, Texas
The Plus Side Of 3D Mammograms
As a clinical researcher and diagnostic radiologist who reads thousands of mammograms each year, I was dismayed to read the KHN investigation “A Million-Dollar Marketing Juggernaut Pushes 3D Mammograms” (Oct. 22), which stated “there’s no evidence they are more effective than traditional screenings.” Hundreds of peer-reviewed scientific articles substantiate improved recall rates and cancer detection rates associated with 3D mammography. This article fails to present this information to readers and causes significant confusion in patients and physicians nationwide.
Recalls ― or “callbacks” — from screening mammography impose a tremendous psychosocial and economic burden on patients. Not only do patients and their families experience fear and anxiety due to a potential cancer diagnosis, but recalls also lead to downstream noncompliance with future screening recommendations and, on average, a 13-month delay to returning to screening mammography. Experiencing a recall or false positive increases the risk of late-stage diagnosis, when breast cancers are larger and harder to treat.
The experience of radiologists reading thousands of mammograms is not anecdotal. It is rooted in evidence-based medicine and data. These are not my opinions, they are facts.
― Dr. Nila H. Alsheik, chair of breast imaging, Advocate Aurora Health Care, Chicago
How High Is High?
The article “Employers Are Scaling Back Their Dependence On High-Deductible Health Plans” (Oct. 29) did not provide enough detail to confirm whether the cost to the employer of the PPO options was the same, more or less than the cost of the “high”-deductible health option. For example, it wasn’t clear whether the employer was making a contribution to the Health Savings Account or Health Reimbursement Account for the high-deductible health option.
Assuming the PPOs and the high-deductible health option all use an 80%-20% coinsurance formula after the deductible up to the same out-of-pocket expense maximum, the employee contributions you quoted give the appearance that the PPO options are much more attractive to almost every employee. For that result to occur, the cost to the employer for the PPO options would have to be substantially greater than the cost to the employer of the high-deductible health option.
Happy Friday! A quick programming note: We are closing up shop for Thanksgiving, so I will be leaving you to your turkey and pumpkin pie next week. But never fear, I’ll be back in your inboxes Dec. 6, as we barrel out an outrageous pace toward the end of the year.
Speaking of outrageous pace, is everyone doing OK after this news-filled week? If you’re feeling stressed you missed something health-related while distracted by the approximately 13 billion big stories going on simultaneously, relax, I’ve got you covered.
One of those 13 billion big stories was, of course, the latest Democratic debate. But the candidates might be feeling some health care fatigue like the rest of us because, although they hit their talking points, they moved quickly on to subjects beyond “Medicare for All.” That came as a slight surprise, since earlier in the week Sen. Elizabeth Warren (D-Mass.) released a plan on how to move more gradually into such a system than she’d previously discussed. Warren’s new blueprint would start by offering a more generous, subsidized government plan for some Americans and pass MFA by the end of her third year.
Meanwhile, California Gov. Gavin Newsom has already walked the fine line that the progressive 2020 candidates are attempting when it comes to universal health care. He also ran on the idea of a single-payer system and has been navigating what happens when political slogan meets reality ever since he was elected. Could his experience offer insight to the Warrens of the world?
The White House was left scrambling this week after President Donald Trump made an unscheduled visit to Walter Reed Medical Center last Saturday. The speculation over Trump’s health spread like wildfire, and the White House’s attempts to frame the trip as Part One of the president’s annual physical were widely mocked by late-night hosts. Officials later shifted the story, saying it was just a routine checkup, but the damage had been done.
Side note (because I was curious, and you might be, too): During his tenure, then-President Barack Obama in 2014 made an unscheduled Saturday trip to Walter Reed, as well. The reason? A sore throat. (h/t WSJ.)
CMS Administrator Seema Verma has said that the hundreds of thousands of dollars spent on outside communications contractors was meant to spread awareness of CMS’ policies. But emails obtained by Politico show that some of the discussions between those contractors and federal officials focused on getting Verma high-profile features in magazines like Glamour, winning recognition for her on “Power Women” lists and getting her invited to attend prestigious events.
In other news, this heartbreaking story takes a look at families of developmentally disabled beneficiaries who are stranded on waitlists because the state slashed its Medicaid funding.
A new Trump administration rule would force hospitals to reveal the prices they negotiate with insurers for all their procedures, as part of a larger strategy to increase transparency in health care. As you might imagine, hospitals and insurers were very much not pleased and have already promised a legal fight. The negotiations have always been shrouded in mystery, and revealing them would be tantamount to exposing trade secrets, they say.
A Wall Street Journal investigation has revealed that 1 in 4 of the doctors involved in the 163 malpractice claims against the Indian Health Service that the government settled or lost since 2006 had a history of medial mistakes and regulatory sanctions that should have raised red flags in the hiring process. At least 66 of the patients died as a result of the alleged malpractice.
The Department of Justice planned to announce a plan Friday to combat chronic and underreported violence against Native American women. The DOJ has faced criticism after past investigations found that thousands of missing-persons cases are missing from the agency’s logs. The proposal includes a plan to hire coordinators across the country who would be responsible for developing protocols for a more coordinated law enforcement response to missing-persons cases.
If you want to get a look at drugmakers’ behavior during the start of the opioid epidemic, look no further than what’s going on in China, apparently. An Associated Press investigation reveals that the tactics being employed there by a Sackler-owned company mirror the ones that spawned a crisis — as well as thousands upon thousands of lawsuits. That includes things like telling doctors that OxyContin is less addictive than other opioids and representing the drug as safe for chronic pain.
Meanwhile, county officials in Ohio struggle with incredibly tough decisions when it comes to reuniting children who were taken away because of a parent’s addiction. If the wrong choice is made it can — and has — ended in the death of a child.
A big, federal study showed that drugs are just as effective at saving lives as surgeries for blocked arteries. But here’s the thing, other studies have already shown this, and yet doctors still perform them. Why? Hint, hint: It just might have something to do with the fact that those procedures pull in the big bucks (though doctors say it’s because past studies were poorly designed).
• South Dakota’s new slogan to combat drug use in the state was thoroughly dragged through the social media wringer this week. “Meth. We’re on it,” was lambasted as both tone-deaf and ridiculous. But, the governor pointed out, it got your attention, didn’t it?
• Who better to take notes from on addiction than Big Tobacco? In the early days, Juul executives were bragging about the “leg up” they got from cigarette research.
• They’re billed as “quiet rooms,” but the isolated timeout spaces found in schools across Illinois seem far more troubling than the name suggests. Children are being kept in these rooms, locked up, alone and terrified — and the practice of doing so is often under-monitored by state officials.
• And so the pendulum swings: As more is discovered about CTE (chronic traumatic encephalopathy) and the neurological damage done by playing football, many youth leagues have been banished. But the cultural roots of the sport run deep, especially in Texas where the game is making a comeback.
Meredith Balogh has spent years learning to navigate the financial side of the health care system.
Balogh, who has Type 1 diabetes, has saved herself and her family many thousands of dollars. She has made a habit — even a hobby — of helping others: people with diabetes, co-workers and strangers on the internet.
“There’s only three things that you’re fighting,” she said. “Problems with competence, problems with greed and problems with maliciousness. And, luckily, most things are incompetence.”
Balogh said she has never had a lot of money, and for years she didn’t have health insurance. But she has become a master at climbing what she calls the “billing info ladder.”
“I do this for fun!” she said, laughing.
She checks in on forums like Reddit’s r/HospitalBills in search of people to help.
Online, Balogh sagely shares her ninja ways for negotiating with a doctor’s office or finding the right thing to say when you call a hospital billing department. Words like “charity care” and “financial aid” are key.
“You are negotiating for your life, be polite ALWAYS, maybe cry a little, but keep asking,” she told one person on Reddit.
Season 3’s Episode 2 of “An Arm and a Leg” begins with Balogh’s story but ends on a personal note: It turns out saving nearly $800 on your medical bill is kinda romantic.
Season 3 is a co-production of Kaiser Health News and Public Road Productions.
In fall 2009, several dozen of the best minds in health information technology huddled at a hotel outside Washington, D.C., to discuss potential dangers of an Obama White House plan to spend billions of tax dollars computerizing medical records.
The health data geeks trusted that transitioning from paper to electronic records would cut down on medical errors, help identify new cures for disease and give patients an easy way to track their health care histories.
But after two days of discussions, the group warned that few safeguards existed to protect the public from possible consequences of rolling out the new technology so quickly. Because this software tracks the medicines people take and their vital signs, even a tiny error or omission, or a doctor’s inability to access the file quickly, can be a matter of life or death.
The experts at that September 2009 meeting, mainly members of the American Medical Informatics Association, or AMIA, agreed that safety should be a top priority as federal officials poured more than $30 billion into subsidies to wire up medical offices and hospitals nationwide.
The group envisioned creating a national databank to track reports of deaths, injuries and near misses linked to issues with the new technology.
It never happened.
Instead, plans for putting patient safety first — and for building a comprehensive injury reporting and reviewing system — have stalled for nearly a decade, because manufacturers of electronic health records (EHRs), health care providers, federal health care policy wonks, academics and Congress have either blocked the effort or fought over how to do it properly, an ongoing investigation by Fortune and Kaiser Health News shows.
Over the past 10 years, the parties have squabbled over how best to collect injury data, over who has the power to require it, over who should pay for it, and over whether to make public damning findings and the names of those responsible for safety problems.
In 2015, members of Congress derailed a long-planned EHR safety center, first by challenging the government’s authority to create it and later by declining to fund it. A year later, Congress stripped the Food and Drug Administration of its power to regulate the industry or even to track malfunctions and injuries.
“A lot of people involved with patient safety and medical informatics were horrified,” said Ross Koppel, a University of Pennsylvania sociologist and prominent EHR safety expert. Koppel said the industry won legal status as a “regulatory free zone” when it came to safety, an outcome he called a “scandal beyond belief.”
The Electronic Health Record Association, a trade group that represents more than 30 vendors, declined to comment on the safety issue.
Meanwhile, patients remain at risk of harm. In March, Fortune and KHN revealed that thousands of injuries, deaths or near misses tied to software glitches, user errors, interoperability problems and other flaws have piled up in various government-sponsored and private repositories. One study uncovered more than 9,000 patient safety reports tied to EHR problems at three pediatric hospitals over a five-year period.
Allegations of EHR-related injuries or other flaws have surfaced in the courts. KHN/Fortune examined more than two dozen such cases, such as a California woman who mistakenly had most of her left leg amputated because the EHR sent another patient’s pathology report indicating cancer to her medical file. A Vermont patient died after a doctor’s order to scan her brain for an aneurysm never made it from the computer to the lab.
Despite such incidents, experts believe EHRs have made medicine safer by eliminating errors due to illegible handwriting and in some cases speeding up access to vital patient files. But they also acknowledge they have no idea how much safer, or how much the systems could still be improved because no one — a decade after the federal government all but mandated their adoption — is assessing the technology’s overall safety record.
KHN and Fortune found that at least a dozen expert commissions, federal health IT panels and medical associations have echoed AMIA’s early call to track EHR safety risks only to be thwarted by objections from the industry or its allies, or by simple bureaucratic inertia. Some critics see the situation as a dispiriting Washington tale of corporate “capture” of government, while others wonder why a warning system to alert health officials to dangers with certain software is even controversial.
“How is it in the public interest for medical records software to have flaws that lead to deaths?” said Joshua Sharfstein, who served as FDA deputy commissioner when the safety issue flared up during President Barack Obama’s first term. These incidents “should be fully understood and investigated” and “not be able to be buried.”
Support for computerizing medical records has spanned the political spectrum. The health IT industry’s aversion to FDA oversight has won support at critical times both with liberals who embraced EHRs as a high-tech magic bullet for reforming the nation’s costly health care system and with free-market conservatives skeptical of red tape and government interventions.
The vendors protested they were overburdened with technical requirements that their software had to meet to qualify for the government subsidy program. Those specifications included many relatively small-bore features, like including a check box indicating the doctor had asked about the patient’s smoking status — and other tasks likely to have little impact on safety.
Complicating things further, many safety advocates themselves have worried that heavy-handed oversight — such as requiring approval of every software update — could actually make the technology less safe, stalling urgent software updates (not to mention stifling innovation and slowing the marketing of vital new technology).
After a contentious process in which consumer advocacy group Public Citizen accused FDA officials of collaborating with the devices industry to weaken oversight, Congress passed the 21st Century Cures Act. A few sentences buried in the law, signed by Obama in late 2016, all but shut the door on FDA regulation of EHRs.
The bipartisan law, which speeds up approvals for some medical therapies, states flatly that electronic health records are not medical devices subject to FDA scrutiny. Some longtime EHR safety advocates say they have all but given up hope for consensus on any system that would investigate and share findings from adverse events, as happens in other industries, like transportation and aviation.
“We have nothing like that,” said Justin Starren, director of the Center for Data Science and Informatics at Northwestern University. “We have the opposite … with vendors saying that customers are explicitly forbidden from publicizing problems they encounter.”
Starren noted that health care providers don’t like to share safety failures either: “It’s the liability fear. If an institution holds up its hand and says, ‘Our EHR might be killing people,’ the lawyers will be lining up outside the courthouse door.”
Less Red Tape Unleashes Red Flags?
In the months before the 2009 AMIA meeting, concern was mounting at the FDA over the rapidly advancing EHR rollout.
Since the mid-1980s, however, the FDA had considered health IT to present a low risk of harm because a “learned intermediary,” such as a doctor, was in charge. Most manufacturers agreed and insisted their products were not medical devices, but vehicles for processing and storing medical information.
The legal distinction is critical. While the FDA requires device makers to report adverse events, the policy in place gave EHR manufacturers a pass. At least one major vendor, Cerner Corp., has concluded that EHRs are, in fact, medical devices and has submitted some error reports to FDA’s public MAUDE database. But most manufacturers disagree and have not reported data, leaving a sizable gap in the agency’s grasp of possible hazards.
Within the FDA, some staffers urged the agency to rethink the hands-off stance given the rush by hundreds of health IT companies — many of them new entrants — to sell medical records software that tens of thousands of doctors, hospitals and patients would rely on.
On Sept. 22, 2009, FDA staff shared their views with deputy commissioner Sharfstein and his boss, commissioner Margaret Hamburg, at a “regulatory strategy” meeting. After hearing the pitch, Hamburg agreed the FDA “needs to be involved in the White House [EHR] initiative,” according to an agency memo. Hamburg had no comment for this article.
One former FDA official recalls tension mounting as the agency became more assertive, saying: “It was a big train going down the tracks at 80 miles per hour, and there were concerns that FDA would slow it down.”
The FDA sounded a public warning at a February 2010 hearing. The agency’s chief devices regulator, Jeffrey Shuren, testified that even with limited surveillance, the FDA had tied six deaths and 44 reported injuries to health information technology failures.
In all, Shuren said, the FDA had logged 260 reports of “malfunctions with the potential for patient harm” over the previous two years. In one case, the software filed results from emergency lab tests to the wrong patient’s electronic record.
Shuren described the reports as likely the “tip of the iceberg” and said they suggested “significant clinical implications and public safety issues.” He laid out three options for FDA involvement, the least burdensome being registration of EHR software and mandatory reporting of dangerous incidents. Through an agency spokesperson, Shuren declined to be interviewed for this article.
Shuren’s 2010 testimony did not appear to carry much weight with David Blumenthal, a Harvard physician chosen as the Obama administration’s point man for the digital medical record rollout. Blumenthal declined to comment.
Many in Blumenthal’s division, known as the Office of the National Coordinator for Health Information Technology, or ONC, sympathized with the industry’s assertion that FDA regulation would discourage innovation, which, in turn, could cripple the president’s plans to revolutionize health care and save money. Blumenthal, who was convinced EHRs would make medicine much safer, described the FDA injury reports as “anecdotal.”
An obscure outpost of the Department of Health and Human Services in the second Bush administration, ONC under Blumenthal revved up as federal officials laid plans for distributing billions of stimulus dollars.
The stimulus law directed ONC to set up two diverse advisory panels so that no single faction of the health care sector could unduly influence policy. Yet it seemed clear, at least to skeptics, that ONC depended heavily on the goodwill, expertise and guidance of the technology community.
(Credit: Fortune)
Steven Findlay, who served on one of the panels as a representative of Consumers Union, said industry witnesses often “commandeered” the discussions because they “had the technical knowledge to steer things in a direction that they wanted.”
Safety “was not necessarily their first priority. They were building products to serve an industry and designing them to make money,” Findlay said in a recent interview.
Dean Sittig, a medical informaticist at the University of Texas Health Science Center at Houston and early researcher on EHR safety, said ONC was “trying to promote” digital records “and there wasn’t a lot of interest in talking about things that could go wrong.” That conflict persists, he said. “They gave out $36 billion. It’s hard for them to say EHRs aren’t safe.”
The ONC did form a safety “working group.” The panel suggested that doctors and hospitals be required to report “potential hazards” and “incidents” to a national database or risk forfeiting government subsidies for purchasing records software, according to minutes from its March 12, 2010, meeting.
That idea never got past the drafting stage, however.
Glitches In The Matrix
In a nod to safety, ONC asked the National Academy of Sciences’ Institute of Medicine to weigh in, a move some at the FDA hoped would at the least lend support for nationwide collection of injury data.
When the 18-member expert panel held a public hearing in mid-December 2010, Shuren reappeared with updated FDA figures — about 370 reports of “adverse events or near misses” involving health IT since January 2008. Once again, he called FDA’s count a “small percentage of the actual [adverse] events that do occur.”
Among the causes he cited: failure of the software to interface properly with other technologies, user errors, design flaws and inadequate pre-market testing.
Shuren suggested EHRs were medical devices over which the FDA “has exercised enforcement discretion; meaning it has not enforced existing requirements,” an apparent reference to the hands-off policy. He called for “real-time collection, aggregation and analysis” of reports on the functioning of EHRs.
The Institute of Medicine panel in November 2011 called on HHS to make adverse incident reporting mandatory for vendors and voluntary for users. It also said HHS should ask Congress to approve a government-run injury monitoring system as rigorous as that used to promote airline safety that would both investigate and make its findings public. The FDA might not be the best-equipped agency to take on the task, the group noted.
The panel asserted that EHR vendors face “competing priorities, including maximizing profits and maintaining a competitive edge, which can limit shared learning and have adverse consequences for patient safety.”
One member called for even stricter oversight. In an impassioned dissent, Richard Cook, a Chicago radiologist and safety expert, argued EHRs were medical devices that necessitated the scrutiny of the FDA.
“At least a few U.S. citizens — perhaps more than a few — have died or have been maimed because of health IT. The extent of the injuries generated by health IT is unknown because no one has bothered to look for them in a systematic fashion,” Cook wrote in his dissent.
(Credit: Fortune)
Backtracking On Oversight
In 2012, Congress required FDA, ONC and the Federal Communications Commission to propose “risk-based” oversight for health IT that “promotes innovation, protects patient safety, and avoids regulatory duplication.”
Two years went by before the agencies did so. In April 2014, they promoted a “limited, narrowly tailored approach” to oversight led by the ONC as well as a “surveillance mechanism” to track adverse events and near misses.
ONC’s budget for the 2015 and 2016 fiscal years proposed spending $5 million for such a center, which ONC said would begin “a robust collection and analysis of health IT-related adverse events.”
But four House Republicans in June 2014 questioned whether ONC had the legal authority to set up the center.
Energy and Commerce Committee Chairman Fred Upton of Michigan, Vice Chairman Marsha Blackburn of Tennessee, health subcommittee Chairman Joseph Pitts of Pennsylvania and communications and technology subcommittee Chairman Greg Walden of Oregon argued that ONC had failed to satisfy their concerns over what Blackburn termed regulatory “mission creep.” At a House hearing in July 2014, Blackburn repeated her worry about “a misguided system of regulation.”
Former ONC director Karen DeSalvo said she was five months on the job and felt completely blindsided by the line of questioning — despite the National Academy of Sciences report years earlier that had advised HHS to seek approval from Congress to expand ONC’s oversight role. The center’s prospects dimmed further when the Congressional Research Service issued a report on the matter in early 2015 that seemed to side with the Republicans.
DeSalvo’s team later requested legislative authority to create the center, but the effort was not successful. ONC was granted legislative authority for other requests, however, empowering it to define interoperability and to crack down on vendors who improperly restrict access to medical records.
These days, many of the key players have conflicting opinions and recollections about what went wrong and why.
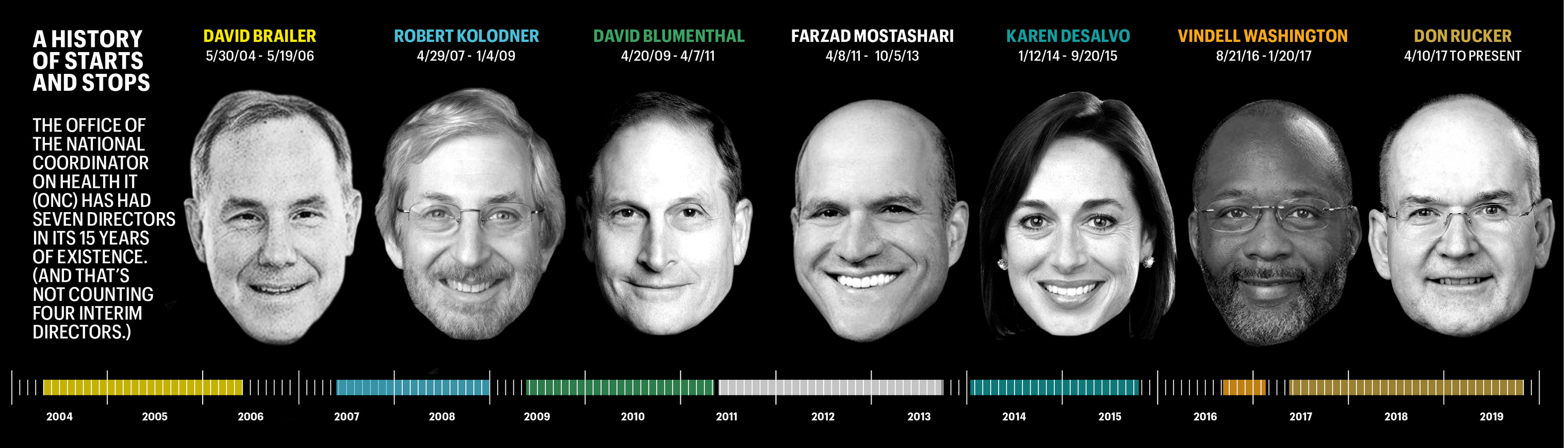
DeSalvo, now a professor of medicine and population health at Dell Medical School, said she really doesn’t know if something sinister torpedoed the safety center or it was just a matter of not enough people caring. “It was really just kind of start and stop,” she said. That’s perhaps not surprising, considering ONC has had seven directors in its 15 years of existence — and six since 2009, when the government made EHRs a national priority. (And that’s not counting four interim directors who collectively helmed the outfit for 16 months.)
Doug Fridsma, who left his role as ONC’s chief scientist in 2014, cited other factors that slowed the center’s momentum. He said uncertainty over its mission didn’t help gain the trust of the industry, while citing other thorny issues, such as who would foot the bill and whether its data might be used to discipline or otherwise harm vendors. Fridsma, now AMIA’s chief executive, said that government-sponsored regional patient safety organizations aren’t well equipped to conduct national oversight of EHR functions.
“It has resulted in a vacuum around health IT safety,” said Fridsma. “Congress has failed to make it a priority.”
Shifting Public Attention
Revisiting plans for a full-fledged EHR safety center holds little appeal to Don Rucker, the Trump administration’s ONC chief.
Rucker said he sees little value in collecting data on incidents often “years and years” after they occurred. Rapidly evolving technologies are making computer errors easier to recognize and remedy. “We can catch these things a lot earlier,” he said.
Rucker argues that the 21st Century Cures Act prohibits the industry from enforcing “gag” clauses that in the past have handcuffed hospitals and doctors from criticizing their EHRs. The Cures law includes fines of up to $1 million for “information blocking,” including taking steps to discourage EHR users from reporting adverse events and other problems for review.
New freedom to sound off assures that doctors and hospitals will begin sharing EHR problems, mitigating any need for mandatory reporting, in Rucker’s view. Rucker said he hopes to have the regulations in place by the end of the year.
The proposed ONC regulations cite a “strong public interest” in “open communication of information regarding health hazards, adverse events and unsafe conditions.” But that information won’t be shared with the public. ONC says all reports of problems are exempt from public release under the Freedom of Information Act. Congress gave these records the same legal status as income tax returns as part of the Cures law.
Jacob Reider, a former ONC interim director, said the government’s failure to do more to promote public awareness of safety concerns is disappointing — and even irresponsible — given its zeal in bringing EHRs into the mainstream of medicine.
“I remember internal conversations where we talked about ‘What is the equivalent of a plane crash that is going to get the attention of people?’” said Reider, who now practices family medicine in upstate New York. “‘Is it going to be a congressperson’s relative is harmed by health IT that causes the attention to shift?’ I would offer that still hasn’t happened yet, but someday it will. And gosh, wouldn’t it be a horrible thing that we have to wait for that to happen?”